Retail Merchandising and Shelf Visibility: Why Shelf Position Is a Revenue Decision, Not a Display Preference
Turn this article into takeaways for your work.
Each assistant summarizes the article only for you and suggests best practices for your work.
Two products, same efficacy, same price, same category. One sits at eye level with four facings and a counter card next to the register. The other is on the bottom shelf, two facings, partially obscured by a promotional display for a competing brand. The first product outsells the second by three to one.
This isn't a marketing story. It's an operations story. And the person who determines which product gets the better position is almost always the field rep who asks for it.
Shelf merchandising is not a nice-to-have or a brand exercise. It's a measurable driver of over-the-counter pull and pharmacist recommendation behavior. Commercial leaders who treat it as a display preference miss the lever entirely. Reps who treat it as a negotiation, one that happens on every visit with data and preparation behind it, compound their revenue advantage visit by visit.
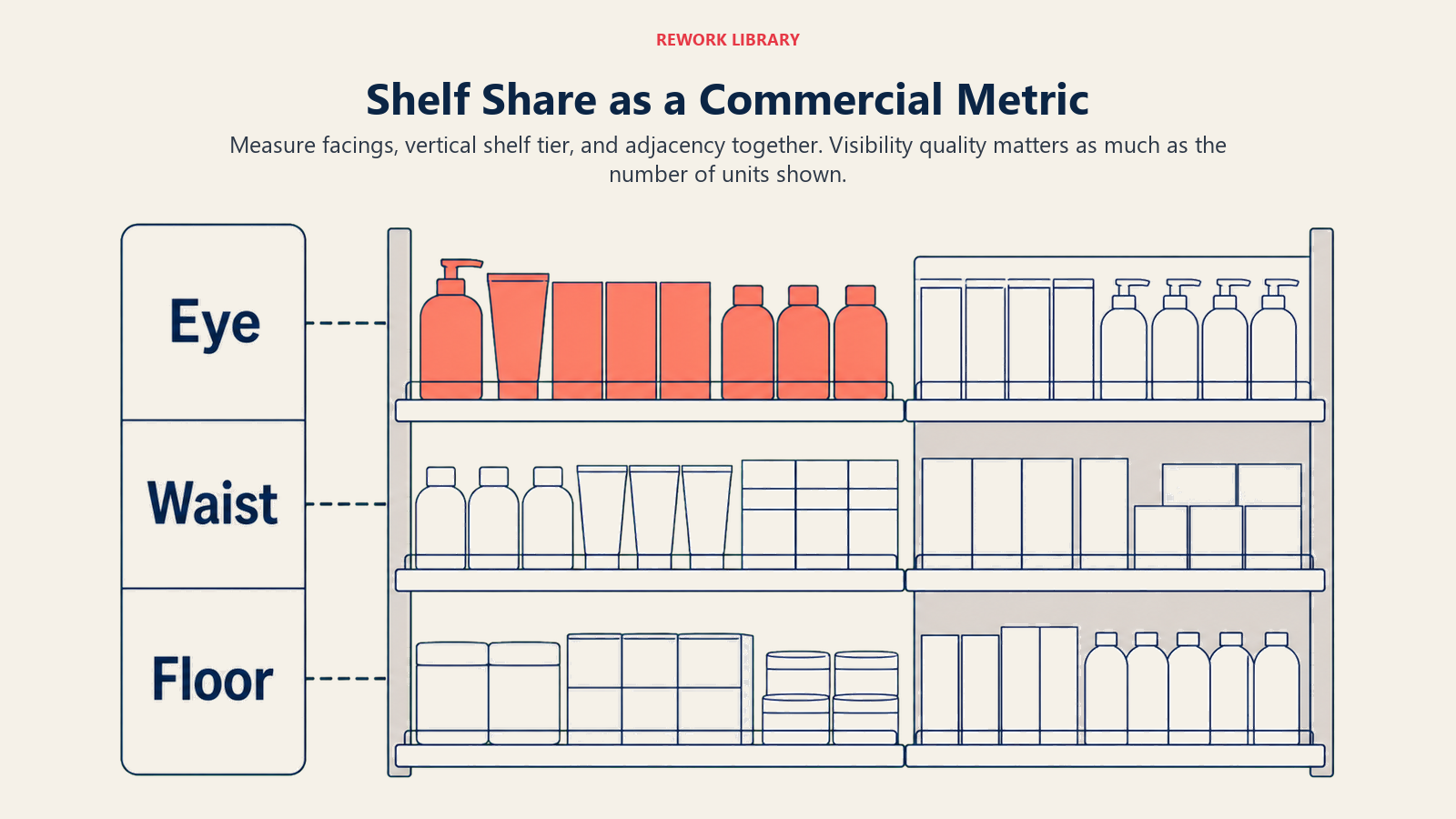
Shelf Share as a Commercial Metric
Before a rep can negotiate shelf position, they need to think about shelf position in commercial terms, because that's the only language that moves a pharmacist.
 Three metrics define shelf share in a pharmacy context:
Three metrics define shelf share in a pharmacy context:
Facing Count: The number of product units visible from the front of the shelf for a given SKU (stock keeping unit). Two facings means two units of your product are immediately visible to a customer scanning the shelf. Four facings means four. More facings increase visual presence and signal to browsers that the product is popular (a proxy for trustworthiness). In most pharmacy categories, the market-leading product holds three to six facings. Matching the leader's facing count is the minimum viable position. Exceeding it on a high-velocity product is a competitive advantage.
Shelf Tier: Eye level (roughly 1.2 to 1.6 meters off the floor) generates disproportionately higher customer engagement than waist level (0.7 to 1.0 meters) or floor level (below 0.7 meters). In-store experiments confirm that middle-shelf positioning consistently generates the highest purchase rates across product categories. Retail research across grocery and pharmacy categories consistently shows that eye-level products outperform floor-level products by two to three times on equivalent facings. The exact differential varies by product category and customer demographics, but the direction is universal.
Adjacency: What your product sits next to matters. Placement adjacent to the category leader implies comparability and benefits from leader traffic. Placement adjacent to a slow mover or unrelated category reduces the quality of shopper engagement. Being blocked by a competitor's POS display is functionally a reduction in visibility even if facing count is unchanged.
| Tier | Height | Illustrative Engagement Index | Notes |
|---|---|---|---|
| Eye level | 1.2 to 1.6 m | 100 (baseline) | Prime position, highest customer engagement |
| Waist level | 0.7 to 1.0 m | 55 to 70 | Acceptable for high brand awareness products |
| Floor level | Below 0.7 m | 20 to 35 | Avoid for OTC prescription-adjacent products |
| Top shelf | Above 1.8 m | 30 to 45 | Visibility poor, reach creates friction |
These index values are illustrative benchmarks based on general retail merchandising principles, not a single published source. The direction is consistent across retail research: products at eye level outperform those at floor or top-shelf positions, often by two to three times on equivalent facings. Chain pharmacy planogram design formalizes these tiers into centrally mandated shelf schematics, which is why understanding the tier framework matters even in independent pharmacy negotiations.
Key Facts: Retail Shelf Visibility
- In-store experiments confirm that middle-shelf positioning consistently generates the highest purchase rates across product categories, with lower-shelf positions producing meaningfully fewer sales on equivalent facings.
- Eye-tracking research in community pharmacies confirms that repositioning OTC products by shelf tier directly changes where customers look and what they select, with gaze duration on repositioned products increasing substantially after environmental redesign.
- Eye level is the highest-value shelf tier in any pharmacy: the engagement gap between eye-level and floor-level products is consistently large across retail categories, which is why moving a product up even one tier is one of the fastest levers available to a rep seeking to improve sell-out without changing price or advertising.
The Merchandising Standard
Every commercial organization needs a clear definition of what a "winning" shelf position looks like for each product in each pharmacy type. Without this standard, merchandising quality is unverifiable. A rep can't audit what they can't measure, and a manager can't hold performance accountable without a benchmark.
A practical merchandising standard for a mid-market OTC product in a retail pharmacy might look like:
Minimum Viable Standard: 2 facings, waist level or above, within the primary category section, no competitor POS blocking.
Target Standard: 3 to 4 facings, eye level, adjacent to category leader or premium positioning, product-branded shelf strip in place.
Gold Standard: 4+ facings, eye level, counter card at point of recommendation (pharmacy counter), window or floor stand for seasonal or promotional periods.
Define the standard by product category and pharmacy segment (independent, small chain, major chain). Different standards apply in different environments because the available shelf real estate and the decision-maker dynamics differ significantly. Once the standard is defined, the real question is how to negotiate for it.
The pharmacy visit playbook should include the merchandising standard for each product as a reference tool reps carry into every call.
How Do You Negotiate Shelf Position Without Planogram Authority?
Most independent pharmacy owners control their own shelf placement. Chain pharmacies operate under centrally mandated planograms. The negotiation approach differs between these environments, but neither is unapproachable.
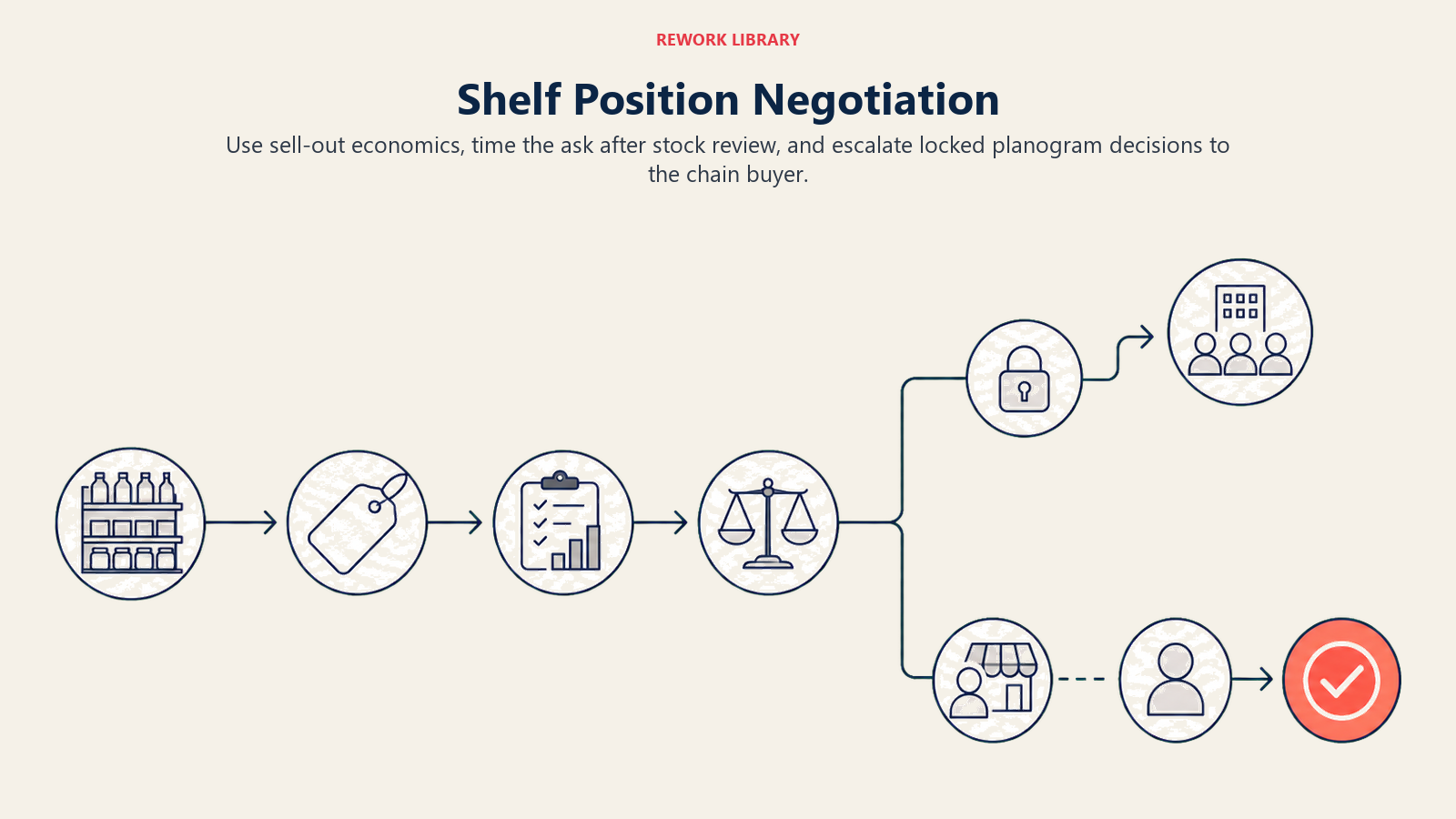
Building the Ask Around Pharmacist Economics
The foundation of every shelf negotiation is the pharmacist's economics, not brand preference or rep enthusiasm.
A pharmacist's economic interest in shelf placement comes down to three things: turnover rate (how fast does the product sell?), margin per unit (what does the pharmacist earn per sale?), and customer satisfaction (does the product solve the customer's problem reliably?). A product that turns quickly at a healthy margin is worth better shelf space. The rep's job is to make that case with data.
"I've tracked your sell-out on [product] over the last three months. You're moving about [units] per week. At your standard margin, that's [gross margin estimate] per week from this product. If we move from two facings on the second shelf to four facings at eye level, retail category data consistently shows meaningful uplift in consumer selection for products moved to eye level. That's incremental contribution from the same square footage."
This is not a pitch. It's a business conversation. Pharmacists respond to numbers because their business runs on numbers. Building the gross margin estimate into the shelf negotiation is essentially the same skill as ROI calculation in B2B sales: the buyer moves when you translate a commercial argument into their own financial terms.
Timing the Ask
The shelf position ask should never open the visit. It should come after stock confirmation and the order conversation, once the pharmacist has already engaged in a business discussion about the product.
Sequence:
- Greet and establish purpose of visit
- Check stock (shelf count, back room)
- Present sell-out data and confirm or place order (see pharmacy order and stock management)
- Transition to merchandising: "While we're talking about [product] performance, I wanted to show you something about the shelf positioning..."
The timing signals that the merchandising conversation is connected to performance, not to the rep's aesthetic preference. It also ensures the pharmacist is already in a business conversation mode rather than a "let me get rid of this rep" mode.
The Graceful Retreat When Position Is Locked
In chain pharmacies, shelf position is controlled by a central planogram that the individual store pharmacist cannot override. When this is the case, attempting to negotiate with the store-level team is wasted effort and can damage the relationship.
The correct response is acknowledgment and escalation: "I understand the planogram controls shelf position here. I'll take this through our key account team who works with your buying office. Is there anything at the store level, counter cards, a shelf strip, anything within your discretion that I can use to improve visibility for customers in the meantime?"
This preserves the relationship, demonstrates understanding of how the business works, and still extracts whatever marginal visibility improvement is available at the outlet level. The key account team handles the planogram conversation with the right decision-maker.
POS Material Placement
Point-of-sale material, counter cards, dispensers, window stickers, and floor stands, can meaningfully amplify shelf visibility or create clutter that the pharmacist removes within days. The difference is placement logic.
Counter Cards and Dispensers
The pharmacy counter is prime real estate. Customers standing at the counter are present, attentive, and often receptive to a pharmacist recommendation. A well-placed counter card at the recommendation moment is a decision-support tool.
Placement rules by pharmacy layout:
- Small independent pharmacy (single counter): Counter card goes to the side of the primary transaction area, visible to the customer but not blocking the pharmacist's workspace. The pharmacist must not feel that the card impedes their professional service.
- Chain pharmacy (dual counter, dispensing plus OTC): Counter card goes on the OTC counter where customer questions and self-selection happen. Avoid placement on the dispensing side where customers collect prescriptions.
- Pharmacy with separate OTC consultation desk: This is the highest-value placement. The pharmacist who uses this desk is already in recommendation mode.
Ask for permission. "Would it be alright if I placed a counter card here? I'll keep it compact, and I'll take it away or replace it when we have new creative." Permission is more reliable than assumption.
Window Stickers and Floor Stands
Window stickers add value during seasonal demand peaks (cold season, allergy season, pain management campaigns) when there is genuine consumer interest in the category driving foot traffic. Outside seasonal relevance, they age quickly and pharmacists discard them.
Floor stands work in pharmacies with defined OTC browsing areas and sufficient floor space. They're irrelevant in compact independent pharmacies where floor space is at a premium. Never place a floor stand where it creates a safety hazard or blocks foot traffic.
POS Placement Decision Matrix:
| POS Material | Best Setting | Avoid When | Permission Needed |
|---|---|---|---|
| Counter card | High-traffic counter with OTC consultation | Counter already crowded, dispensing-only counter | Yes, always |
| Shelf strip/talker | Own shelf section | Competitor POS occupies section | Store discretion |
| Floor stand | Defined OTC browsing area, 2m+ clearance | Compact pharmacy, no OTC aisle | Yes, always |
| Window sticker | Seasonal peaks, front-facing pharmacy | Non-seasonal period, high-prestige pharmacy | Yes, ask first |
| Dispenser/clip strip | Near complementary category | Where it looks out of place | Yes, always |
Shelf Audit on Every Visit
The shelf audit takes sixty seconds. It should happen on every visit, documented with specific data rather than impressions.
The audit captures six things:
- Facing count by SKU: Count the actual number, don't estimate. Record in CRM.
- Shelf tier: Which level is the product on? Has it moved since last visit?
- Competitor facing count and tier: Relative position matters as much as absolute position.
- Adjacency: What brands flank your product? Has this changed?
- POS material status: Is the counter card still in place? Is the shelf strip legible? Has it been covered or removed?
- Competitor encroachment: Has a competitor product expanded into your facing space or positioned POS material near your product?
Sixty seconds of structured observation catches changes that reps who simply glance at the shelf routinely miss. Competitor encroachment on shelf position is common and rarely announced. A rep who doesn't audit systematically loses position gradually across a territory.
Shelf Audit Scorecard (per visit):
| Element | Current Status | vs. Last Visit | Action Required |
|---|---|---|---|
| Facing count | |||
| Shelf tier | |||
| Competitor facings | |||
| Adjacency (left/right) | |||
| Counter card in place | |||
| Shelf strip legible | |||
| Overall position: Win / Hold / Lost |
Fill this during the visit. Log it in the CRM before leaving the pharmacy.
Chain Pharmacy vs. Independent Pharmacy Merchandising Dynamics
The decision-maker for shelf position is different in each environment, and the rep's approach needs to reflect that difference.
Independent Pharmacy: The pharmacist owner or senior manager makes placement decisions, often in real time. They're motivated by personal business economics and customer loyalty considerations. They respond to data about their own customers, their own sell-out rates, and their own competitive context. Relationship capital built over multiple visits translates directly into shelf preference.
The independent pharmacy is where a rep's merchandising skill has the highest immediate impact. A well-prepared rep with three months of sell-out data and a clear business case for eye-level placement can win a position upgrade in a single visit. Eye-tracking research in community pharmacies confirms that repositioning OTC products by shelf tier directly changes where customers look and what they select.
Chain Pharmacy: The individual outlet operates under central planogram direction. Shelf position, facing count, and adjacency are determined by a category management team at headquarters based on scan data, trade terms, and supplier agreements.
At the outlet level, the rep can influence what falls within store discretion: counter card placement, seasonal POS material, and verbal advocacy from the store pharmacist to the buying team. At the headquarters level, the key account team negotiates planogram position, promotional allocations, and category captain status.
Understanding the independent vs. chain pharmacy strategy for your organization determines where each merchandising effort should be directed.
The pharmacy relationship management framework matters differently in each context. In independent pharmacies, relationship drives shelf preference directly. In chain pharmacies, relationship drives in-store execution quality (POS placement, pharmacist advocacy) but not planogram position.
Photography and Reporting
Shelf photography serves two commercial purposes: documentation of current position for territory management, and evidence of wins and losses for commercial analysis.
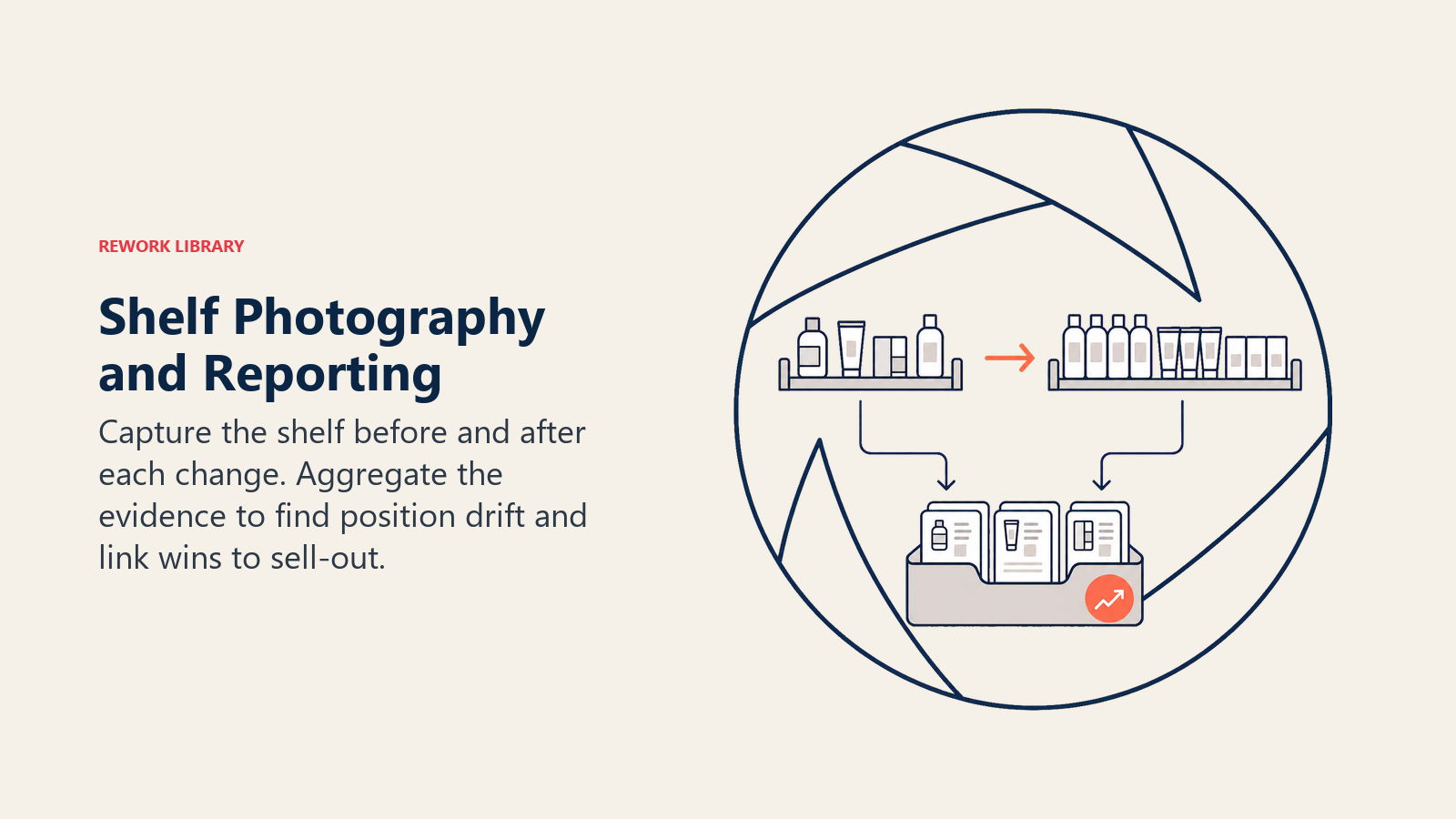 The documentation practice is simple. On every visit, photograph the shelf section containing your product before any changes are made. Label the photo with the pharmacy name, date, and SKU. After any changes (additional facings, position upgrade, POS placement), photograph again. The before-and-after record shows the change achieved and creates accountability for maintaining it on the next visit.
The documentation practice is simple. On every visit, photograph the shelf section containing your product before any changes are made. Label the photo with the pharmacy name, date, and SKU. After any changes (additional facings, position upgrade, POS placement), photograph again. The before-and-after record shows the change achieved and creates accountability for maintaining it on the next visit.
The commercial analysis purpose is more strategic. Aggregated shelf photography from across a territory, analyzed by region and product, reveals patterns: which pharmacy segments are responding to merchandising investment, where competitor products are gaining position, and which rep behaviors correlate with better shelf share outcomes.
Secondary sales tracking and pull-through data aligned with shelf audit records can show whether position improvements are driving the sell-out increases the business case predicted. This closes the loop and justifies continued investment in merchandising activity at the territory level. The same logic applies to pipeline velocity analysis in sales operations: measuring the rate at which opportunities convert, not just the number of opportunities open, reveals which inputs actually move the needle.
Reporting expectations vary by organization, but a minimum viable standard is: one shelf photograph per visit logged to CRM, monthly territory-level shelf audit summary shared with the field manager, and any competitive encroachment events flagged within 24 hours. The reps who do this consistently are the ones who catch position drift before it becomes position loss.
Frequently Asked Questions about Retail Merchandising and Shelf Visibility
What shelf tier should I target for my OTC product?
Eye level, defined as roughly 1.2 to 1.6 meters off the floor, is the highest-value position in any pharmacy shelf set. Retail category research consistently shows that eye-level products outperform floor-level products by a significant margin on equivalent facings, and waist-level positions fall somewhere between the two. If you can only achieve one merchandising improvement in a visit, moving from the bottom or top shelf to eye level has more impact than adding facing count at a poor tier.
How do I negotiate shelf position with a pharmacist who doesn't want to change their display?
Ground the negotiation in the pharmacist's economics, not your brand preference. Calculate the gross margin contribution of your product at current turnover, then estimate what a meaningful increase in consumer selection (consistent with what retail category research shows for eye-level versus lower-shelf positioning) would add in weekly contribution. Present that as a business case rather than a brand request. Frame the ask around what is good for their dispensary. Pharmacists who manage by the numbers respond to numbers.
What can I do about shelf position in a chain pharmacy with a central planogram?
At the store level, focus on what falls within the individual pharmacist's discretion: counter card placement, seasonal POS material, and a shelf strip within your existing section. None of these require planogram approval. For actual position changes, escalate through your key account team to the category buyer or commercial team at the chain's head office. Attempting to negotiate planogram position with a store-level pharmacist who lacks that authority wastes both your time and damages the relationship.
How often should I conduct a shelf audit, and what should I document?
Shelf audits should happen on every visit, not periodically. The audit takes sixty seconds and captures six elements: facing count by SKU, shelf tier, competitor facing count and tier, adjacency (what flanks your product), POS material status, and any competitor encroachment on your facing space. Document the results in your CRM before leaving the pharmacy. The trend across three to six visits reveals position drift that a single-visit observation misses entirely.
What POS materials generate the most value in pharmacy settings?
Counter cards at the pharmacy consultation counter have the highest value because they place your brand at the exact moment a pharmacist is interacting with a patient. Floor stands work in pharmacies with defined OTC browsing areas and adequate floor space. Window stickers add value during seasonal demand peaks when category interest is high. None of these materials generate lasting value if placed without permission: always ask first, and commit to replacing or removing materials at the next visit. A pharmacist who was asked and agreed will protect your display; one who didn't is likely to remove it.
How does shelf visibility connect to prescription pull-through?
A pharmacist who can see your product, who has it at a position that makes it easy to reach and hand to a patient, is more likely to recommend it at the dispensing counter. When product is on the bottom shelf partially obscured by a competitor display, the path from prescription to dispensed brand requires extra effort from the pharmacist. Visibility removes that friction. Secondary sales tracking data aligned with shelf audit records can show whether position improvements are driving the sell-out increases the business case predicted.
The Shelf Share Audit System is the core merchandising method this article describes: on every visit, capture facing count, shelf tier, competitor position, adjacency, and POS material status, and log all six data points in the CRM before leaving the pharmacy. The system converts shelf observation from an impression ("it looks okay") into a tracked metric with a trend line. That trend line is what tells a rep whether they are holding, winning, or losing position visit by visit, and it gives the commercial manager visibility across the territory without relying on self-reported estimates.
Two additional points are worth carrying into every shelf conversation. Eye-tracking research in community pharmacies confirms that tier changes alter actual customer gaze behavior, not just theoretical selection probability. And planogram authority in chain environments is not a wall: it is a routing instruction. The shelf negotiation for chain accounts belongs at the category buyer level, and the in-store conversation should focus entirely on what that store-level pharmacist actually controls.
Conclusion: Shelf Position Is Negotiated Visit by Visit
There's no such thing as a permanently won shelf position. A product that holds four eye-level facings today can lose two of them to a competitor who simply asked for them on the next rep's visit after yours.
Shelf position is negotiated continuously. Every visit is an opportunity to hold what you have, recover what you've lost, and advance where the pharmacist's business case supports the ask. The rep who treats the shelf as static, returning to the same position visit after visit without auditing, isn't managing merchandising. They're just walking by it.
Commercial leaders who want to improve retail pull-through need to build shelf audit and merchandising negotiation into the field team's core operating rhythm, not as optional best practice but as a tracked, reported activity with defined standards and visible accountability. The sell-through data will show the difference.
Learn More

Senior Implementation Consultant
On this page
- Shelf Share as a Commercial Metric
- The Merchandising Standard
- How Do You Negotiate Shelf Position Without Planogram Authority?
- Building the Ask Around Pharmacist Economics
- Timing the Ask
- The Graceful Retreat When Position Is Locked
- POS Material Placement
- Counter Cards and Dispensers
- Window Stickers and Floor Stands
- Shelf Audit on Every Visit
- Chain Pharmacy vs. Independent Pharmacy Merchandising Dynamics
- Photography and Reporting
- Conclusion: Shelf Position Is Negotiated Visit by Visit
- Learn More