Rep Onboarding, Training, and Coaching: Building a High-Performance Pharma Field Force

Turn this article into takeaways for your work.
Each assistant summarizes the article only for you and suggests best practices for your work.
The first 90 days set a medical rep's performance ceiling. Not their CV. Not their interview score. Not the strength of the territory you hand them. How you onboard, train, and coach them in that window shapes every habit, every health care professional (HCP) relationship, and every territory behavior they'll carry for the next three years.
Most pharma sales organizations underinvest here. They run a week of product training, drop a rep into the field with a senior buddy for a few days, and then expect results by month three. The rep scrapes through with a partial grasp of the product portfolio, limited clinical knowledge, and a coaching relationship that amounts to a manager glancing at their call reports every fortnight.
The companies that build high-performance field forces treat onboarding and coaching as an operational system, not a one-time event. This guide gives pharma sales directors and first-line managers a structured framework to do exactly that.
Why the First 90 Days Determine a Rep's 3-Year Trajectory
A new rep who lands in territory with insufficient product knowledge doesn't just underperform. They build bad habits.
Key Facts: Rep Onboarding and Attrition
- Industry estimates for replacing a medical rep, including recruiting, onboarding, and lost territory revenue during ramp, range from one to two times annual compensation depending on specialty; for a rep earning $100,000 base, total replacement exposure typically runs $100,000 to $200,000
- Reducing time-to-productivity by four weeks across a 200-rep field force with average annual quota of $800,000 per rep represents approximately $10 to 12 million in recovered revenue, depending on the assumed productive selling-day mix within those four weeks
- Research published in PMC on pharmaceutical rep and physician interactions found that skeptical, evidence-oriented specialists respond strongly to reps who arrive prepared with clinical data and methodology, not just headline results (PMC1876413, PLoS Med, 2013)
They learn to deflect clinical questions rather than engage them. They develop workarounds instead of skills. And those patterns calcify. A rep who reaches month six still avoiding certain HCP types or certain product topics is almost impossible to fundamentally retrain without starting from scratch.
The business case for structured onboarding is straightforward. Reducing time-to-productivity by four weeks per rep, across a field force of 200 reps carrying average annual quota of $800,000 each, translates to roughly $10 to 12 million in recovered revenue (at approximately 85% productive selling days within that four-week window). That's before accounting for the cost of early attrition, which spikes dramatically in organizations with weak onboarding programs.
The first 90 days also set the coaching relationship. A first-line manager who establishes clear performance expectations, structured observation cycles, and a development-oriented feedback culture in month one will find those norms accepted and even welcomed. But a manager who tries to introduce rigorous coaching to a rep who's been autonomous for six months will meet resistance.
How Should Pharma Organizations Structure the First 90 Days?
The 90-Day Phased Ramp Model divides new rep onboarding into three distinct phases: foundation week (compliance, product, and territory orientation), field immersion weeks two through four (observed calls and supervised solo work), and a supervised ramp-up from day 30 to 90 (structured coaching observations, monthly knowledge assessments, and formal certification sign-off before independent territory work).
Onboarding Program Architecture
A 90-day onboarding program has three distinct phases, each with different objectives and activities.

Week 1: Foundation
| Day | Activity | Owner |
|---|---|---|
| Day 1 | Company culture, mission, org structure, administrative setup | HR and line manager |
| Day 2 | Regulatory and compliance orientation: promotional claims rules, adverse event reporting, sample management | Medical/Regulatory Affairs |
| Day 3 | Therapy area overview: disease biology, patient journey, unmet need | Medical Science Liaison |
| Day 4 | Product portfolio: approved indications, mechanism of action, key clinical data, formulary status | Training team |
| Day 5 | Territory overview: target account list, A/B/C segmentation, predecessor rep handover notes | Line manager |
Week 1 is not a time for the rep to be in the field. Reps who start calling on HCPs before they can discuss the product's mechanism of action are a compliance and credibility risk. The ABPI Code of Practice requires that representatives in the UK be formally examined on all training units within one year of beginning promotional activities and must achieve full qualification within two years, a standard that makes structured week-one orientation non-negotiable.
Weeks 2 to 4: Field Immersion
- Ride-alongs with experienced peers: The new rep observes a strong performer's call structure, detailing technique, and objection responses. Aim for at least 8 to 10 observed calls before any solo work.
- Territory handover: Walk the geographic territory with the predecessor or line manager. Identify A-account relationships that need immediate repair, pharmacy relationships that carry product stocking influence, and hospital target access patterns.
- CRM system training: Hands-on setup of Veeva, IQVIA OCE, or equivalent platform. Account profiles reviewed for each target. First-week call logging practice under supervision before the rep logs independently.
- Regulatory documentation: Sample management sign-off, promotional materials clearance confirmation, and consent forms for any digital rep interactions.
By end of week four, the rep should be making supervised solo calls. They're not yet fully independent, but they can open, detail, handle a basic objection, and close a call without needing the manager to rescue them.
Days 30 to 90: Supervised Ramp-Up
This is where most onboarding programs collapse. Week-four competence creates the illusion of readiness, and managers pull back too early.
Days 30 to 60 should include:
- A minimum of two joint field visits per week, structured around specific learning objectives (not just presence)
- Formal call observation using a structured scorecard (see coaching section below)
- Monthly knowledge assessment: 20-minute verbal quiz on product data, competitive landscape, and objection responses
- A 30-day performance review against call activity, call quality scores, and initial coverage metrics
Days 60 to 90 transition to a less intensive but still structured cadence:
- One joint field visit per week, with rep leading and manager observing
- 60-day ramp milestone review (are they hitting 80% of expected call activity? Are key A accounts covered?)
- Introduction to territory analytics: how to read their own performance data
- 90-day certification sign-off on product knowledge and detailing competency
Medical Knowledge Certification Standards
Pharma reps operate in a regulated promotional environment. A rep who makes an off-label claim, overstates efficacy data, or is unable to answer a basic safety question from an HCP creates legal exposure for the organization and credibility damage to the brand.
Medical knowledge certification should cover:
Clinical dossier depth: Can the rep explain the primary and secondary endpoints of the pivotal trial? Can they describe the patient population studied? Do they know the number needed to treat for the primary endpoint? These aren't advanced questions. They're table stakes for a specialist-facing rep.
Regulatory-approved claims: The rep must know which claims are approved for promotion and which aren't. This includes understanding how to handle HCP requests for information that falls outside the approved label. The answer is almost never to volunteer the data in a promotional context. But the rep needs to know the correct response. The OIG Compliance Program Guidance for pharmaceutical manufacturers identifies training on regulatory-approved claims as one of the seven elements of an effective compliance program, and off-label promotion is among its primary identified risk areas.
Competitor landscape: Know the competitor products in the category, their approved indications, their key clinical data, and their market positioning. A rep who doesn't know the main competitor's mechanism of action will lose credibility in a specialist conversation within the first three minutes.
Selling Skills Training Modules
Medical knowledge without selling skills produces reps who can talk about the product but can't move a prescriber. Selling skills training should cover four core modules:
Detailing technique: Opening with a patient scenario rather than a product feature, transitioning from unmet need to mechanism of action, presenting evidence in a way that's clinical rather than promotional, and closing with a specific ask ("Would you be comfortable trialing this for your next three patients with Stage 2 disease?"). Doctor detailing best practices provide a structured framework for this. Reps who also train in SPIN selling develop a sharper diagnostic instinct, using situation, problem, implication, and need-payoff questions to uncover what actually drives an HCP's prescribing decision before presenting any data.
Objection handling: This isn't about scripted rebuttals. It's about understanding why HCPs object (safety concerns, formulary barriers, habit, competitor preference, previous negative experience) and responding with data and empathy rather than pressure. Pre-call planning and objection handling should be built into rep preparation as standard practice.
Relationship building with HCPs: GPs respond to reps who make their life easier (clear messages, relevant patient resources, respectful of time). Specialists respond to reps who are clinically credible and can discuss data. Pharmacists respond to reps who understand their business model. Training reps to adapt relationship approach by customer type isn't manipulation. It's professionalism.
Relationship building with pharmacists: Pharmacists have significant patient contact and can influence adherence, switching, and OTC recommendations. Reps who treat pharmacy visits as box-ticking exercises miss a high-yield touchpoint. Train reps to discuss patient counseling opportunities, not just stocking levels.
Field Coaching Cadence
Coaching is not feedback. Feedback is telling someone what they did wrong. Coaching is working with someone to build the capability to do it better. First-line managers who understand this distinction build better reps and retain them longer.
Frequency Benchmarks by Tenure
| Rep Tenure | Joint Field Visits per Month | Observation Type |
|---|---|---|
| Months 1 to 3 | 8 to 10 | Double-blind ride-along and structured scoring |
| Months 4 to 6 | 4 to 5 | Manager observes rep independently |
| Months 7 to 12 | 2 to 3 | Selective observation, development focus |
| Year 2 and beyond | 1 to 2 | Development and retention focus |
"Double-blind ride-along" means the HCP knows someone is visiting with the rep but doesn't know who's being assessed. This produces more natural rep behavior than formal "manager is watching" calls, which often produce show performances that don't reflect daily execution.
Structured Observation and Feedback Form
A good coaching observation scorecard covers:
| Dimension | What to Observe |
|---|---|
| Pre-call preparation | Did the rep review last call notes? Were materials ready? |
| Opening | Patient scenario or challenge opener vs. product introduction opener |
| Needs identification | Did the rep ask about current prescribing patterns before presenting? |
| Key message delivery | Was the core message clear, evidence-based, and aligned to HCP's patient profile? |
| Objection handling | Did the rep listen, acknowledge, and respond with data or empathy? |
| Close | Was there a specific, patient-level ask? |
| Post-call | Was CRM updated promptly? Was a follow-up committed? |
Score each dimension 1 to 5. Identify one strength and one development focus per call. Never try to address five things at once after a coaching observation. One clear development priority, discussed with examples, and followed up at the next joint visit.
The Coaching Conversation
After an observed call, the manager's first question should always be: "How do you think that went?" A rep who accurately self-assesses is developing judgment. A rep who consistently over-rates their own performance has a self-awareness gap that needs to be surfaced gently but directly.
The coaching conversation structure:
- Positive observation: specific behavior, not generic praise. Not "great call" but "the way you referenced her specific patient profile before presenting the data worked really well. She leaned in."
- Development area: specific behavior, not character. Not "you need to be more confident" but "when she raised the tolerability question, you moved on quickly. Next time, let's try sitting with that objection and exploring it with the data before you transition."
- Commitment: what will the rep do differently in the next call? Make it specific and observable.
The Role of the First-Line Manager
The distinction between coaching and telling is the central competency difference between a strong pharma field manager and a weak one.
Telling sounds like: "You need to open with the patient scenario, not the product. Do it like this." It might fix the immediate behavior. But it doesn't build the rep's underlying understanding of why the patient scenario opener works. The next time the rep faces a different clinical context, they'll default to their instinct rather than an adapted skill.
Coaching sounds like: "When you opened with the product, how did the doctor respond?" (She looked a bit detached.) "What do you think was going through her mind?" (Maybe she'd heard it before?) "Right. What would have engaged her faster?" (Maybe if I'd talked about the patient type she sees first?) "Exactly. Try that in the next call and tell me what changes."
The rep who arrives at the insight themselves retains it. And the manager who builds that habit of inquiry develops reps who can self-coach. That's how you get a territory ceiling that keeps rising rather than plateauing.
Motivational frameworks for field managers should recognize that medical reps are motivated by a mix of clinical credibility, territory ownership, and recognition. A rep who sees their HCPs improving patient outcomes with their product doesn't need a cash incentive to stay engaged. They need a manager who notices and acknowledges the link between their field work and patient results.
Digital Learning Tools
In-field time is expensive. Digital learning tools extend training capacity without pulling reps off the road:
E-learning modules: Short, scenario-based modules covering objection types, clinical data updates, and detailing technique variations. Fifteen-minute modules that a rep can complete on a tablet between calls are more effective than two-hour classroom sessions that happen twice a year.
Closed-loop marketing feedback integration: When a rep plays a digital detail on an approved device, the CRM captures what content the HCP engaged with, how long they spent on each slide, and what they skipped. This data feeds back into coaching conversations. A manager who can say "your oncology targets are skipping the pharmacokinetics slide" has a specific coaching direction.
Simulation-based product training: Role-play simulations where reps practice objection scenarios in a digital environment before taking them to real HCPs. These tools aren't a replacement for live practice, but they build baseline competence that reduces the number of coaching visits needed to achieve call-ready standard.
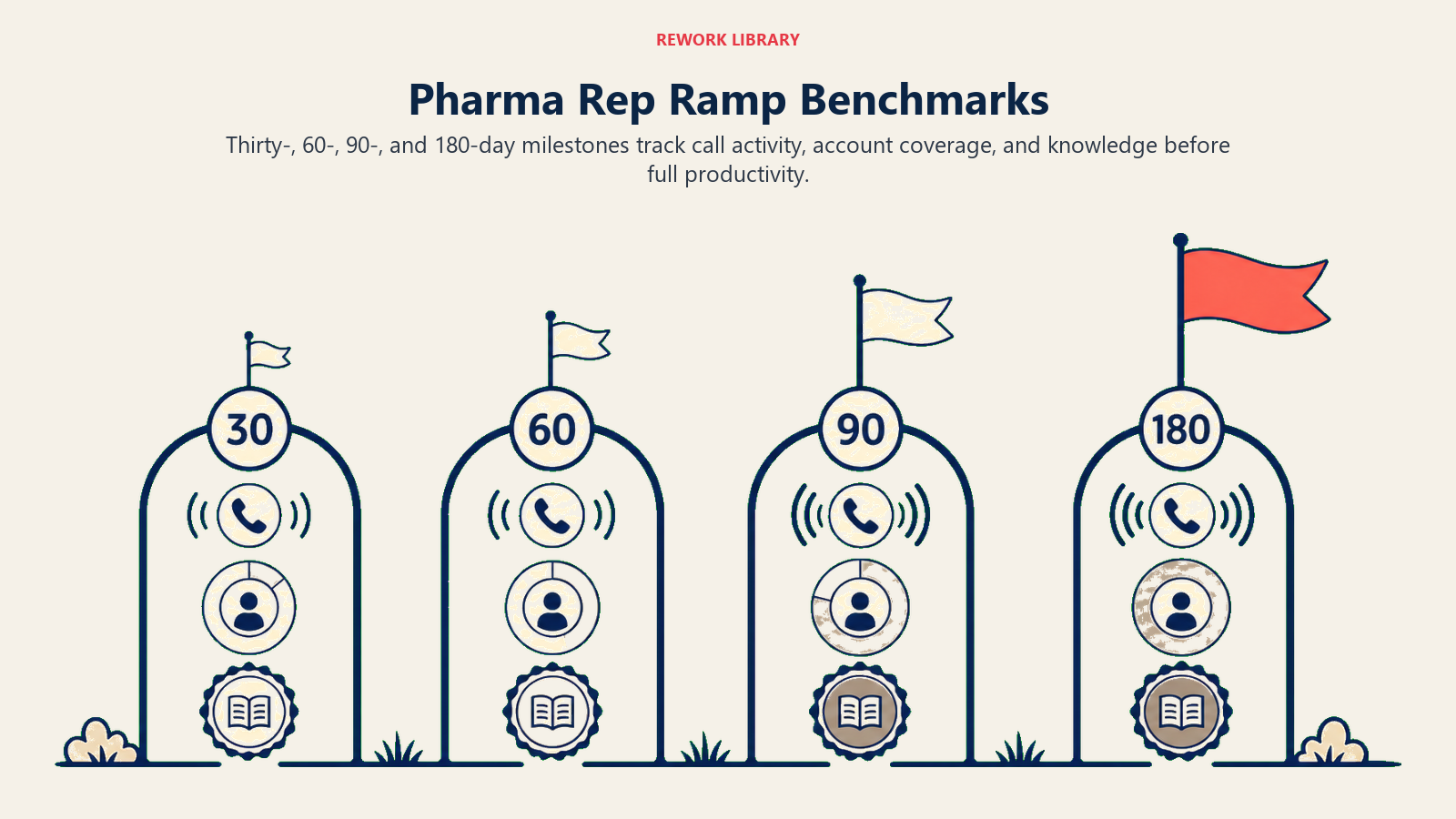
Performance Ramp Benchmarks
Setting clear expectations at each ramp milestone gives reps a target and gives managers an early-warning system for reps who are struggling:
| Milestone | Call Activity | Coverage | Knowledge |
|---|---|---|---|
| 30 days | 60% of target daily call rate | 30% A accounts contacted | Pass basic product knowledge quiz (70%) |
| 60 days | 80% of target daily call rate | 50% A accounts with at least one quality call logged | Pass advanced clinical data quiz (75%) |
| 90 days | 90% of target daily call rate | 70% A accounts with at least two quality calls | Detailing competency sign-off by manager |
| 180 days | 100% of target | Full A/B coverage per territory plan | Independent certification complete |
A rep who misses the 30-day call activity benchmark without a clear explanation (territory access issues, system setup delays) should trigger an immediate support conversation. Don't wait until 60 days to discover that a rep has been struggling with CRM confidence for a month. These ramp benchmarks also feed directly into sales capacity planning: a 90-day ramp window needs to be baked into headcount models, or new territories will carry full productivity assumptions they can't yet meet.
The medical rep daily call plan framework gives new reps a concrete structure to operate within during ramp, rather than learning daily time management by trial and error. And field force sizing and deployment decisions should account for ramp time: a new rep territory shouldn't carry full productivity expectations for the first 90 days.
Building a Learning Culture That Retains Reps
High-performing pharma field forces have one thing in common beyond good onboarding: they've created an environment where learning is continuous, not episodic.
This means:
- Monthly team call discussions where reps share objection responses that worked and those that didn't
- Senior reps who are recognized for developing junior reps, not just for their own territory numbers
- Clinical knowledge updates that go to reps as competitive intelligence, not just as compliance announcements
- First-line managers who make coaching visits feel like development time, not surveillance
Reps who feel supported in developing clinical credibility and selling capability stay longer. Replacement costs for a medical rep (recruiting, onboarding, and lost territory revenue during ramp) are substantial, commonly estimated at one to two times annual compensation. A coaching culture that reduces annual attrition from 15% to 10% across a 200-rep field force saves several million dollars per year in replacement exposure alone.
The ABPI Code of Practice requires that UK pharmaceutical representatives be formally examined on all training units within one year of beginning promotional activities and achieve full qualification within two years, making structured initial training a regulatory requirement, not a preference.
First-line managers who establish structured observation cycles in month one find those coaching norms accepted and embedded. Managers who try to introduce rigorous coaching to reps who've been autonomous for six months consistently meet resistance. Research published in PMC on pharmaceutical rep and physician interactions documents how reps strategically adapt to different physician types: skeptical, evidence-oriented specialists are approached with clinical reprints and engaged as peers, while relationship-oriented GPs respond to a different profile entirely. The implication for onboarding is direct: reps trained to read and respond to physician type outperform those who apply the same approach to every call. The team that builds that credibility early compounds it into prescribing loyalty that competitors find very hard to displace.
Frequently Asked Questions about Rep Onboarding, Training, and Coaching
What is the minimum duration for new medical rep onboarding before field deployment?
The first week should be entirely classroom and office-based: compliance orientation, therapy area briefing, product dossier training, and territory handover. Reps who start calling on HCPs before they can explain the product's mechanism of action create both compliance risk and credibility damage that's difficult to reverse. The ABPI Code of Practice sets a formal examination standard within one year of starting promotional activities, but operational best practice is to certify basic product knowledge before the rep makes any unsupervised calls.
How many joint field visits should a first-line manager do with a new rep?
Eight to ten observed calls during the first four weeks, followed by eight to ten manager-accompanied visits per month through month three, and four to five per month during months four through six. Beyond month six, two to three per month is appropriate for a developing rep, with the focus shifting from competency building to performance refinement. Managers who pull back to one monthly visit before the rep has certified their detailing competency consistently produce reps who develop avoidance habits around the call types they find hardest.
What should be on a rep's certification checklist at 90 days?
The 90-day certification should confirm: product knowledge (primary and secondary endpoints of the pivotal trial, patient population, number needed to treat), detailing competency (scored observation of a full call sequence including opening, evidence presentation, objection handling, and close), regulatory knowledge (approved claims, off-label handling, sample management), and call activity (90% of target daily call rate with 70% A-account coverage). Missing any of these at 90 days should extend supervised ramp, not trigger a pass.
What is the difference between a ride-along and a coaching visit?
A ride-along is observation without feedback: the manager watches the rep's calls without intervening, then provides structured feedback afterward. A coaching visit is more active: the manager and rep may role-switch mid-session, with the manager modeling a technique the rep is developing. The distinction matters because reps who always have the manager available to rescue difficult calls never build the confidence to handle them independently. The first two weeks of onboarding warrant ride-alongs for observation and feedback calibration; from month two onward, coaching visits that build specific skills outperform pure observation.
How should performance ramp benchmarks be set for a new rep territory?
Thirty-day benchmarks should be based on realistic activity expectations, not full quota projections: 60% of target daily call rate and 30% A-account contact at 30 days, scaling to 90% call rate and 70% A-account coverage at 90 days. Full territory productivity expectations should not apply until day 180. Field force sizing and capacity models that assign full quota to a rep from day one consistently produce either sandbagged quotas or demoralized reps who spend their first quarter failing against targets they couldn't realistically hit.
How does digital e-learning fit into a pharma rep training program?
E-learning works best for content that benefits from repetition and self-pacing: objection scenario practice, clinical data review, regulatory compliance refreshers. Short scenario-based modules of 10 to 15 minutes that a rep can complete on a tablet between calls are more effective than two-hour classroom sessions held twice a year. But digital learning doesn't replace live coaching: simulation-based practice builds baseline competence, and live observation with feedback is what converts competence into consistent field behavior.
Learn More
Build a complete field-force capability system with these resources:

Senior Implementation Consultant
On this page
- Why the First 90 Days Determine a Rep's 3-Year Trajectory
- How Should Pharma Organizations Structure the First 90 Days?
- Onboarding Program Architecture
- Week 1: Foundation
- Weeks 2 to 4: Field Immersion
- Days 30 to 90: Supervised Ramp-Up
- Medical Knowledge Certification Standards
- Selling Skills Training Modules
- Field Coaching Cadence
- Frequency Benchmarks by Tenure
- Structured Observation and Feedback Form
- The Coaching Conversation
- The Role of the First-Line Manager
- Digital Learning Tools
- Performance Ramp Benchmarks
- Building a Learning Culture That Retains Reps
- Learn More