Customer Segmentation and Targeting in Pharma Field Sales: Directing Rep Time to the Highest-Value Accounts

Turn this article into takeaways for your work.
Each assistant summarizes the article only for you and suggests best practices for your work.
Equal effort across all accounts is the fastest way to leave revenue on the table in pharma field sales.
When every pharmacy, every doctor, and every hospital gets the same visit frequency regardless of their prescription volume or purchase potential, you're running a field force on fairness principles rather than commercial logic. The rep spends the same time in a pharmacy that moves 10 scripts a month as in one that moves 200. The health care professional (HCP) who hasn't changed her prescribing in three years gets the same detail as the one who's actively building a new patient panel.
The math doesn't work. And the reps who are spending time in low-value accounts aren't spending it in high-value ones.
Segmentation is how you fix this. It's the analytical layer that separates accounts by potential, assigns call frequency and resource allocation by tier, and ensures that the hours your field force has available are concentrated where they'll generate the most return.
Segmentation Dimensions for Pharma
Not all accounts segment the same way. Pharmacies, HCPs, and hospitals have different value drivers, and your segmentation model needs to reflect that.
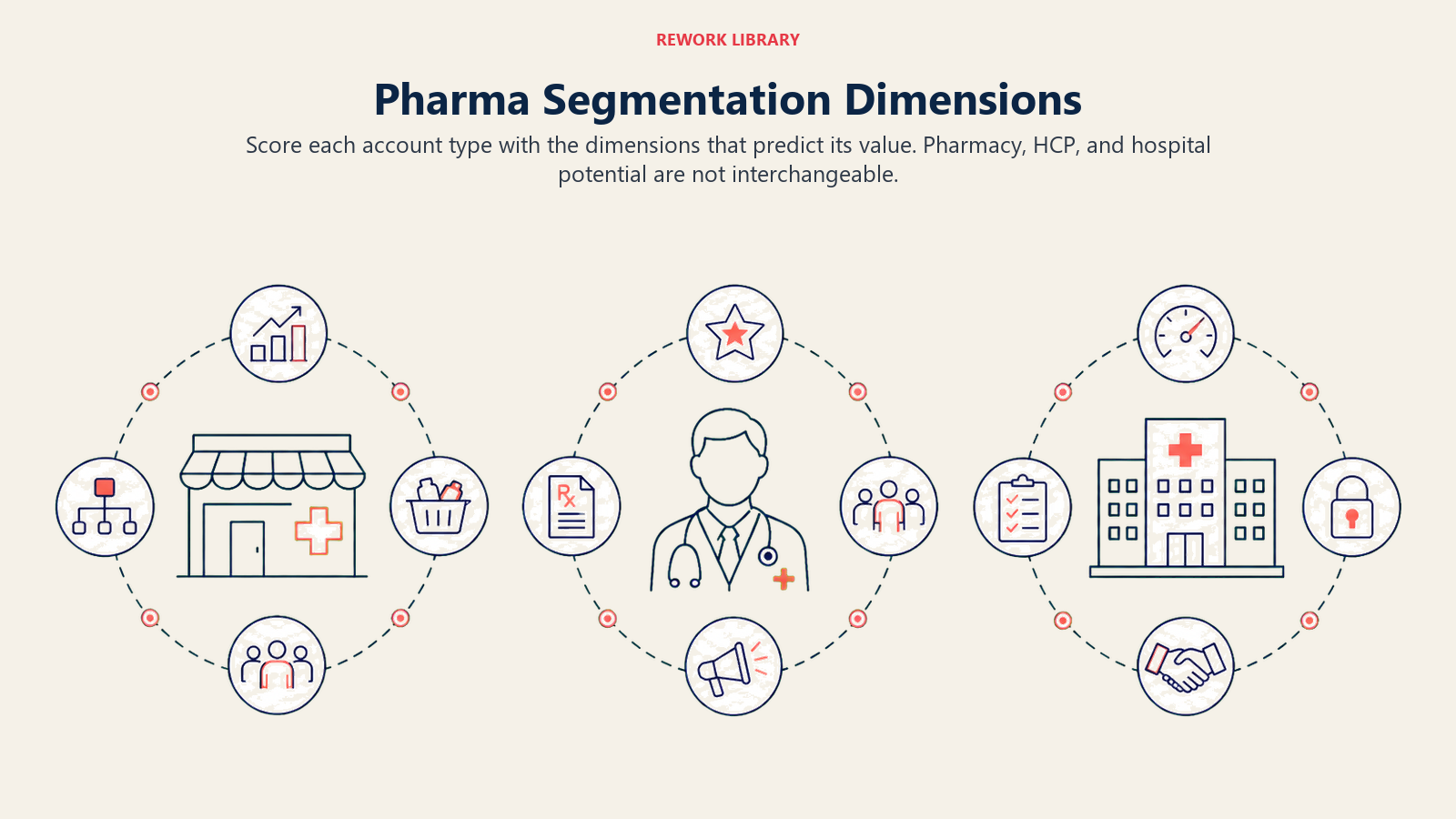
Pharmacies and Drug Stores
The primary segmentation dimensions for pharmacy accounts:
Monthly purchase volume: The most direct indicator of current value. How much product does this pharmacy buy from your distributor or directly from your company? High-volume pharmacies move product regardless of rep attention. Low-volume ones may or may not have growth potential.
Basket mix: What share of the pharmacy's prescription volume is in your therapeutic category? A pharmacy with high total volume but low category penetration may be capturing prescriptions that aren't being filled with your brand. That's a targeting opportunity.
Footfall and patient density: Pharmacy footfall (prescription count and OTC customer traffic) indicates potential demand. High-footfall pharmacies in residential areas near clinics often serve concentrated patient populations for specific conditions.
Chain vs. independent: Chain pharmacy accounts often have centralized buying decisions, which means rep engagement may need to happen at both the store level (with the pharmacist) and the account management level (with the chain's procurement team). Independent pharmacies give the rep more direct influence over purchasing decisions but require more individual relationship effort.
HCPs and Doctors
For physician accounts, the relevant dimensions shift:
Specialty: A specialist in your target therapeutic area is categorically more valuable than a generalist, unless your product addresses a condition that generalists manage first-line. Specialty determines which HCPs can even drive your prescription volume.
Prescribing habit: Within a specialty, individual prescribing patterns vary enormously. IMS/IQVIA data or prescription audits (where available in your market) allow you to identify physicians who are already prescribing in your category vs. those who aren't yet engaged. A high-prescribing HCP who isn't prescribing your brand is a different opportunity from one who doesn't prescribe in the category at all.
Patient panel size: Larger patient panels mean more prescribing occasions. A busy urban GP with 50-60 patient consultations per day represents a very different targeting priority than one with 15-20 consultations, even within the same specialty.
Formulary influence: Some HCPs carry disproportionate influence over prescribing behavior in their hospital department, clinic network, or peer group. These KOLs (key opinion leaders) are often worth targeting above what their individual prescription volume would suggest, because shifting their behavior shifts their network's behavior.
Hospitals
Hospital accounts require a distinct segmentation lens:
Bed count and patient throughput: Larger hospitals see more patients, but bed count alone doesn't tell you about therapeutic area relevance. A 500-bed general hospital may see fewer patients relevant to your brand than a 200-bed specialty center.
Therapy area access: Does your product have access to the relevant inpatient or outpatient department? Is it on the hospital formulary? Unrestricted formulary access multiplies the value of an HCP within that hospital. A formulary restriction or a requirement for specialist initiation changes the targeting calculus.
Tender participation: Many hospital markets operate on annual or biannual drug tenders. A hospital that participates in tenders for your product category is a strategic account that requires coordinated engagement beyond standard rep calls, typically involving medical affairs, market access, and sales leadership.
Key Facts: Pharma Segmentation Impact
- IQVIA prescriber-level data allows identification of physicians prescribing in a therapeutic category at the molecule level across most major commercial markets.
- Deloitte research on biopharma field effectiveness highlights that where reps allocate their limited customer-facing time is a primary driver of commercial results.
- The IQVIA OneKey database covers more than 25 million healthcare professionals and 6 million organizations across 117 countries, enabling potential scoring at the individual HCP level in most major markets.
Building Tier Criteria
Once you've defined the segmentation dimensions, you need decision rules that translate scores on those dimensions into tier assignments. The tier system is what turns an analytical model into operational call planning. The key is defining the attributes that make an account worth prioritizing before you allocate rep time, rather than discovering high-value accounts by accident through broad coverage.
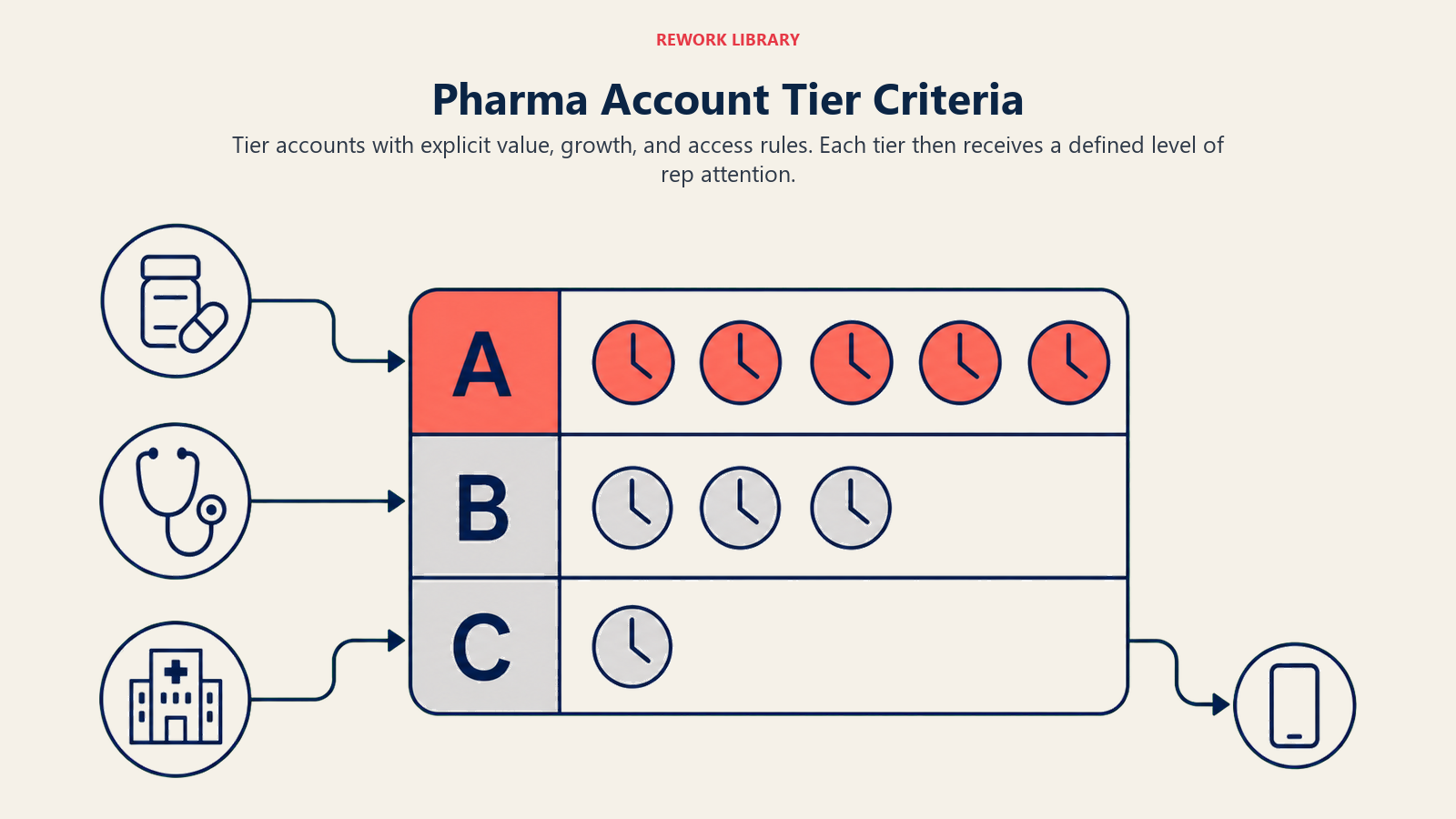
Tier A (High Priority, High Frequency)
Tier A accounts have high current value, high growth potential, or both. For pharmacies, this means top quartile monthly purchase volume in the territory, with category mix indicating upside. For HCPs, it means high prescribing volume in the therapeutic area, with current brand share below their potential. For hospitals, it means unrestricted formulary access and high patient throughput in the relevant department.
These accounts get the most rep time, typically monthly or biweekly calls, and receive the most complete detail including new clinical data, promotional programs, and relationship development activities.
Tier B (Medium Priority, Standard Frequency)
Tier B accounts show moderate current value with identifiable growth potential. A pharmacy in the second quartile of purchase volume that's in a growing catchment area. An HCP with a mid-size patient panel who's newly entering your prescribing category. A hospital with partial formulary access where a relationship investment could improve access over time.
These accounts receive regular calls, typically every six to eight weeks, with standard promotional detail and relationship maintenance.
Tier C (Low Priority, Maintenance or Digital)
Tier C accounts have low current value and limited near-term potential. This doesn't mean they're written off. It means they don't merit the same field investment as Tier A and B accounts. Many Tier C accounts are best served through digital engagement, periodic call drops, or bundled into efficient routing where a rep passes through anyway.
Segmentation Criteria Matrix
| Dimension | Tier A (High) | Tier B (Medium) | Tier C (Low) |
|---|---|---|---|
| Monthly Rx / purchase volume | Top 20-25% of territory | Middle 40-50% | Bottom 25-35% |
| Category penetration | High: strong therapy area presence | Moderate: some category scripts | Low: minimal category presence |
| Brand share vs potential | Underpenetrated: clear conversion opportunity | Partially developed | Fully developed or structurally limited |
| HCP prescribing index | Top decile for specialty | Mid-range prescribers | Low volume or non-prescribers |
| Account access | Open access, responsive to rep | Standard access, occasional barriers | Limited access, rarely converts |
| Strategic value | Formulary influence, anchor account, KOL | Growing influence, referral potential | Stable maintenance relationship |
Data Inputs for Segmentation
Segmentation is only as good as its data. The common trap is building a sophisticated model on data that's two years stale or systematically incomplete.
Secondary sales and prescription data (IMS/IQVIA): This is the gold standard for pharma segmentation where available. IQVIA's prescriber-level data allows you to see prescribing volume by HCP and pharmacy at the molecule level, giving you both current value scores and market share estimates. Not every market has full IQVIA coverage, and data licensing costs vary significantly, but where it's available, it should drive tier assignment. The scoring approach mirrors lead scoring systems used in B2B sales: assign weighted scores to behavioral and firmographic signals, set tier thresholds, and let the model determine call priority rather than relying on rep intuition alone.
CRM historical visit and order data: Your CRM holds call history, sample records, and order data for the accounts your reps have been visiting. This data is valuable for understanding relationship depth, call responsiveness, and historical trends, but it only covers accounts already in your system. Don't let it define the ceiling of your account universe.
Distributor sell-through data: Where your products move through distributor networks, sell-through reports show actual product movement by outlet. This is often the most current picture of pharmacy purchasing behavior, since distributor data updates weekly or monthly rather than quarterly.
Rep-reported field intelligence: Quantitative data doesn't capture everything. Reps know which HCPs are retiring, which pharmacies have changed ownership, which hospital departments have new heads with different prescribing philosophies. Structured field intelligence collection, through call notes, rep surveys, or periodic territory reviews, adds qualitative context that pure data misses. Which targeting model you choose next determines how you use that combined picture.
Targeting Models
The Value-Velocity-Access (VVA) Targeting Model is a practical composite framework: Value scores the account's prescription or purchase potential; Velocity scores the rate of change in that potential (growing, stable, or declining); Access scores the practical rep ability to engage the account (open access, gated, or closed). Tier assignments combine all three, so a high-Value account with poor Access and declining Velocity sits differently than one with the same Value score but improving Velocity and open Access. The three-factor model prevents over-indexing on current volume at the expense of directional opportunity.
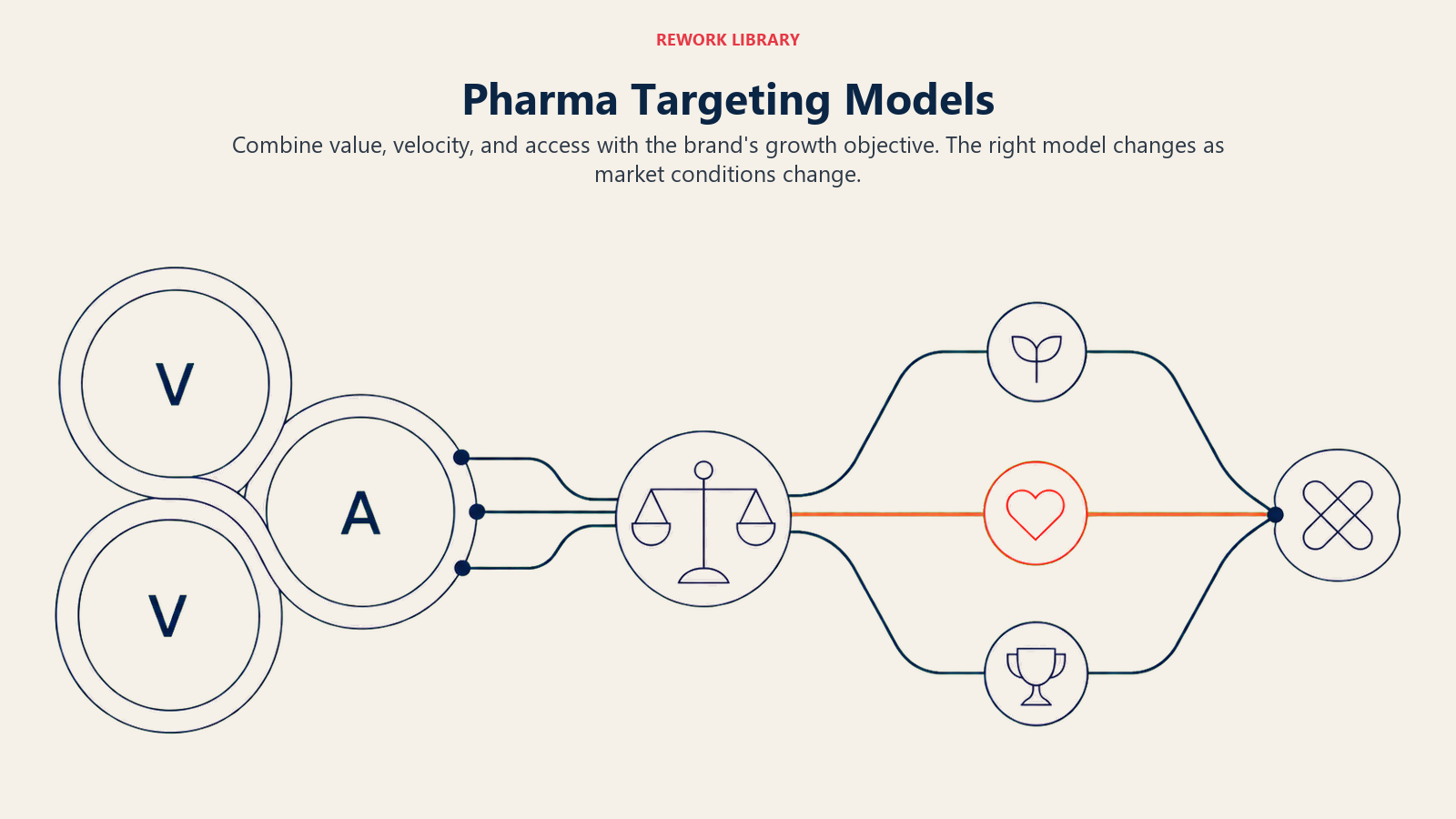
There's more than one way to use segmentation data to direct rep time. Different targeting models reflect different commercial priorities.
Potential-based targeting directs resources toward accounts with the highest absolute prescription or purchase potential, regardless of current brand penetration. The logic: if you're only capturing a small share of a high-volume account, there's more to gain there than in a lower-potential account where you already dominate.
Loyalty-adjusted targeting weights rep effort toward accounts that are already responsive to your brand, on the premise that converting loyal accounts to higher volume is more efficient than acquiring entirely new ones. This model tends to be more conservative, protecting existing share rather than aggressively pursuing new volume.
Competitive opportunity targeting focuses rep time on accounts where your competitors are strong but your brand has differentiated clinical positioning. The goal is conversion, particularly in therapeutic areas where prescribing habit is relatively fixed and competitive displacement is the primary growth lever.
Targeting Model Comparison
| Model | Best Used When | Core Metric | Risk |
|---|---|---|---|
| Potential-based | New launch, underpenetrated market | Total category volume | Spreads reps thin chasing high-potential accounts that may be competitor-loyal |
| Loyalty-adjusted | Mature brand, defending share | Brand share stability | Underinvests in growth accounts, misses conversion opportunities |
| Competitive opportunity | Differentiated brand, defined competitive accounts | Competitive share in target accounts | Requires strong data on competitive prescribing |
| Hybrid | Most steady-state situations | Weighted composite score | Complexity in scoring and tier boundary decisions |
Most commercial teams end up with a hybrid approach: a composite score that weights potential, current performance, and competitive situation, with the weights reflecting where the brand is in its lifecycle.
A high-prescribing HCP who is not yet prescribing your brand represents a fundamentally different commercial opportunity than a high-prescribing HCP who already prescribes it at scale. Potential-based targeting, which directs resources toward accounts where your brand share is below what the account's volume would suggest, consistently outperforms volume-only targeting in penetration-stage brands because it concentrates rep effort on the accounts where behavioral change is most commercially valuable.
Maintaining Segment Accuracy
Segmentation done once and never updated is worse than no segmentation, because it creates false confidence. An HCP who was Tier A three years ago may have retired. A pharmacy that was Tier C may have moved to a new location in a high-traffic area and doubled its volume. A hospital that was Tier B may have added a new specialty unit that's now relevant to your brand.
Quarterly review triggers are the minimum standard for most markets. The review doesn't require rebuilding the model from scratch. It focuses on accounts where field intelligence or data signals indicate the tier assignment may no longer be accurate.
Common triggers for tier review:
- New secondary sales data release (IQVIA quarterly updates)
- Rep-reported changes in account status (HCP departure, pharmacy relocation, ownership change)
- Significant change in regional competitive activity
- New product launch that changes the relevant HCP or pharmacy profile
Rep-reported field intelligence needs a structured mechanism to feed back into the segmentation model. A rep who calls on an account weekly has information no data system captures. Build a simple field intelligence process into your CRM workflow, whether through call note tags, a quarterly territory review form, or a structured debriefing with field managers.
Without this feedback loop, the central segmentation model and the rep's actual experience of their accounts diverge over time. You end up with reps who ignore the tier assignments because they know they're wrong. The next question is how you translate a working segmentation model into actual call plan decisions.
Linking Segmentation to Call Plans
Segmentation only creates commercial value when it drives call frequency decisions. A tier assignment sitting in a spreadsheet that doesn't translate into how a rep plans their week has accomplished nothing.
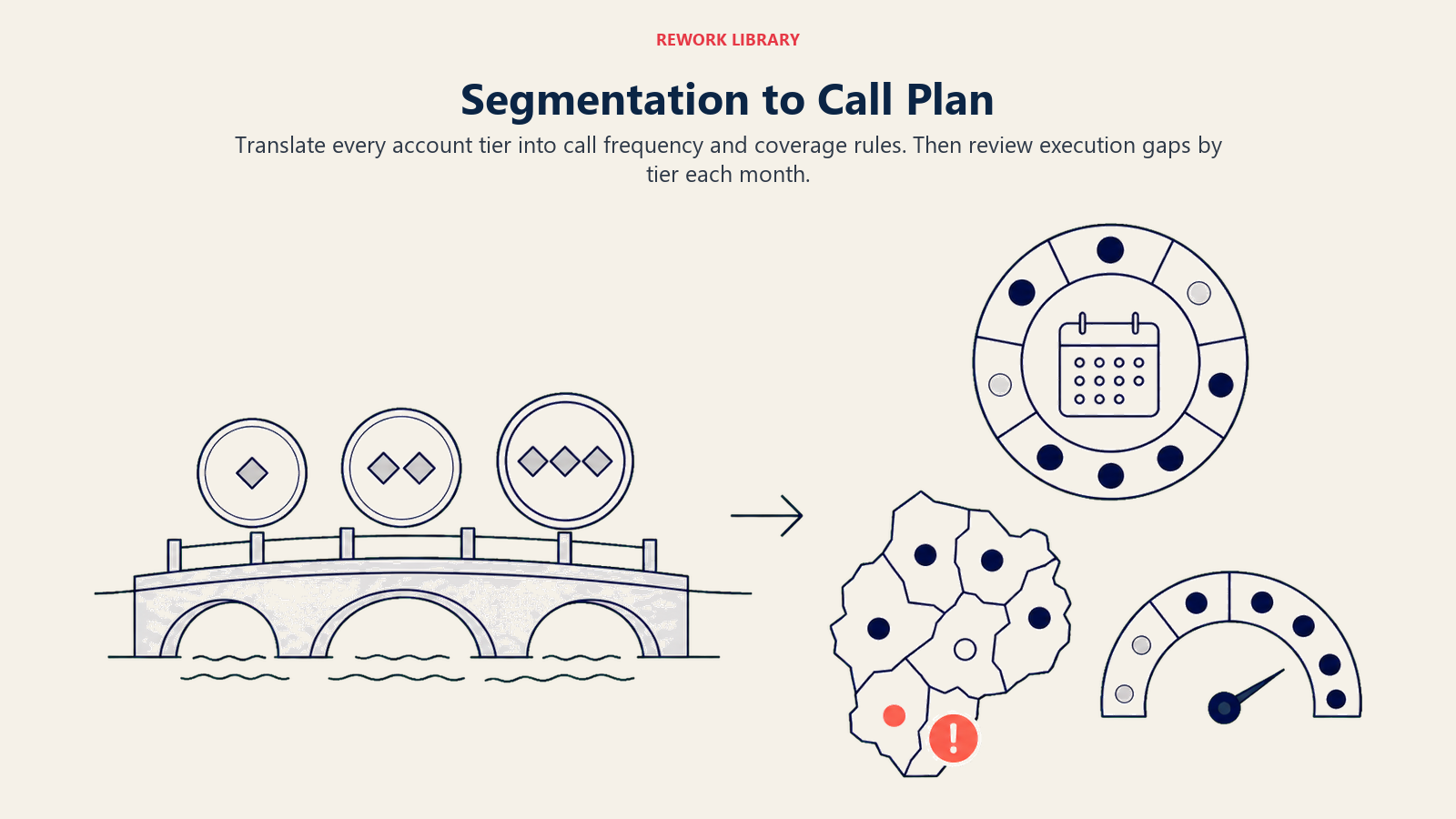 The translation from tier to call plan works through frequency standards and coverage rules:
The translation from tier to call plan works through frequency standards and coverage rules:
| Tier | Target Annual Calls | Calls Per Quarter | Minimum Coverage Rate |
|---|---|---|---|
| Tier A | 12-24 | 3-6 | 95% of accounts |
| Tier B | 6-8 | 1.5-2 | 90% of accounts |
| Tier C | 2-4 or digital | 0.5-1 | 70-80% of accounts |
Coverage rate is as important as frequency. A high-frequency target means nothing if 30% of Tier A accounts aren't being called at all because the rep is spending time in Tier C accounts. Given that Deloitte's research found biopharma reps spend roughly two-thirds of their workday on non-customer-facing tasks, the limited customer-facing time available makes account prioritization the primary lever on commercial results.
Field managers should review coverage reports by tier at least monthly. Persistent coverage gaps in Tier A accounts are a management issue, whether the root cause is territory design, routing inefficiency, or rep prioritization behavior. For call plan execution mechanics, see Medical Rep Daily Call Plan.
The link between segmentation and Call Frequency and Coverage Optimization is direct: segmentation sets the priority order; coverage optimization determines how to execute against that priority order within the practical constraints of geography and time.
Segmentation also drives prospecting strategy. When you know which account types and profiles represent Tier A potential, you know what you're looking for in new accounts. New Pharmacy and Drug Store Acquisition and New HCP Doctor Prospecting become focused exercises rather than broad net-casting.
Precise Segmentation Converts Rep Hours into Revenue
The field force is a finite resource. Every rep has a set number of productive hours per week, and every one of those hours is spent somewhere. At the scale of the global pharmaceutical market, the difference between disciplined and undisciplined account prioritization compounds into substantial revenue variance. Segmentation determines whether those hours are systematically concentrated in the accounts that can move the most product, or spread indiscriminately across accounts of wildly varying potential.
Broad coverage without targeting builds mileage, not revenue. The reps who cover the most ground aren't necessarily the reps who sell the most. The reps who spend the most time in the right accounts are.
That's what segmentation delivers: not a ranking exercise, but a resource allocation discipline. And in a field-force model where headcount costs are largely fixed and the only variable is where those people spend their time, allocation discipline is the primary commercial lever available to commercial leaders.
The territory design that maps the account universe (see Sales Territory Mapping and Account Universe) gives you the geographic container. Segmentation tells you what matters most within it. Together, they're the analytical foundation that makes everything else, routing, call planning, promotional prioritization, measurably more effective.
Frequently Asked Questions about Customer Segmentation and Targeting in Pharma Field Sales
What is customer segmentation in pharma field sales?
Customer segmentation in pharma is the process of classifying accounts (pharmacies, HCPs, hospitals) by their prescription volume, purchase potential, and commercial characteristics, then assigning call frequency and resource allocation based on those classifications. Its purpose is to concentrate rep time where it generates the highest return rather than distributing effort equally across all accounts regardless of their value.
What are the main segmentation dimensions for HCP accounts?
The primary dimensions are specialty (does this HCP prescribe in your therapeutic area), prescribing habit (how many prescriptions do they write in your category and how does your brand share compare), patient panel size (how many relevant patients do they see per day or week), and formulary influence (do they shape prescribing behavior in their network or hospital department). KOLs who carry peer influence are often worth targeting above what their individual prescription volume suggests.
What is the difference between potential-based and loyalty-adjusted targeting?
Potential-based targeting directs reps toward accounts with the highest absolute prescribing opportunity regardless of current brand penetration, prioritizing accounts where share is underbuilt relative to volume. Loyalty-adjusted targeting concentrates effort on accounts already responsive to your brand, converting loyal accounts to higher volume rather than pursuing new ones. Most commercial teams use a hybrid: a composite score that weights potential, current performance, and competitive situation based on where the brand sits in its lifecycle.
How often should segmentation data be refreshed?
Quarterly review is the minimum standard for most markets. Review triggers include new IQVIA data releases, rep-reported changes in account status (HCP departure, pharmacy relocation, ownership change), significant regional competitive activity, and new product launches that change the relevant account profile. Without a structured feedback mechanism from field intelligence into the central model, tier assignments and rep experience of actual accounts diverge over time, leading reps to ignore the model because they know it's wrong.
What call frequency should Tier A accounts receive?
Tier A accounts, defined as high prescription volume or high purchase potential with identifiable conversion opportunity, typically receive 12 to 24 calls per year (monthly to biweekly). Coverage rate is as important as frequency: Tier A accounts should have a minimum 95% coverage rate, meaning nearly all of them receive at least one call per quarter. Persistent coverage gaps in Tier A accounts are a management issue requiring territory, routing, or prioritization intervention.
What is the biggest risk in pharma segmentation models?
The biggest risk is building a sophisticated model on stale or systematically incomplete data, then treating it as the current truth. An HCP who was Tier A three years ago may have retired. A pharmacy that was Tier C may have moved to a high-traffic location and doubled its volume. A hospital may have added a new specialty unit that's now therapeutically relevant. Segmentation done once and not maintained creates false confidence that's often worse commercially than having no formal model at all.
Learn More

Senior Implementation Consultant