Medical MSL and Commercial Alignment: Navigating the Science-Sales Boundary in Pharma

Turn this article into takeaways for your work.
Each assistant summarizes the article only for you and suggests best practices for your work.
There's a scene that medical affairs leaders know well. The medical science liaison (MSL) has spent eight months building a genuine peer relationship with a leading cardiologist: journal club discussions, real-world evidence review, advisory board involvement, honest scientific exchange without any promotional agenda. The key opinion leader's (KOL's) clinical opinion about the product is favorable. They're using it in the patient population where the data is strongest, and they're speaking about it at regional conferences.
Then the sales rep gets their quarterly territory target, learns the cardiologist is a high-decile prescriber, and books an appointment to ask for more scripts.
The KOL calls the MSL afterward. "I thought you were different from the sales people," they say.
That's the medical-commercial alignment failure at its most damaging. The MSL's investment in credibility, built on the premise of independent scientific exchange, is compromised in a single commercial visit. The KOL relationship doesn't disappear immediately, but it shifts from peer trust to cautious distance. The commercial asset that the MSL built is diminished.
Getting medical-commercial alignment right isn't just a compliance requirement. It's a commercial strategy.
What MSLs Do and Why They Sit in Medical, Not Commercial
Medical Science Liaisons are field-based scientific experts who engage health care professionals (HCPs), KOLs, and health system decision-makers on clinical and scientific content that goes beyond what a promotional representative can discuss.
Key Facts: MSL Independence and Commercial Value
- FDA regulations governing pharmaceutical promotion draw a clear line between promotional activities, which must be consistent with the approved label, and scientific exchange, which can cover broader context including investigational data when requested by a healthcare professional (FDA OPDP: https://www.fda.gov/about-fda/cder-offices-and-divisions/office-prescription-drug-promotion-opdp).
- The OIG Compliance Program Guidance for Pharmaceutical Manufacturers identifies manufacturer compensation relationships with physicians connected to marketing and sales activities as a documented fraud and abuse risk area (OIG: https://oig.hhs.gov/documents/compliance-guidance/799/050503FRCPGPharmac.pdf).
- The PhRMA Code on Interactions with Health Care Professionals sets the industry standard requiring that every MSL-HCP touchpoint serve patient care rather than advance a promotional objective, reinforcing why structural separation of MSL and commercial functions is an FDA-guidance expectation and industry best practice.
MSL conversations typically cover: clinical trial methodology and data interpretation, real-world evidence from registry studies or observational data, pharmacoeconomic evidence relevant to formulary or health technology assessment, disease education outside the indication, and post-approval safety monitoring.
The MSL sits in the medical affairs function, not in commercial, for reasons that are regulatory, strategic, and best-practice.
Regulatory and structural: FDA regulations governing pharmaceutical promotion draw a clear line between promotional activities (which must be consistent with the approved label and may only reference approved indications) and scientific exchange (which can cover broader scientific context including investigational data when requested by a healthcare professional). The MSL's ability to engage in those broader scientific conversations depends on their independence from promotional intent. If MSLs report to commercial leadership, receive sales-based incentives, or take direction on call content from commercial teams, that independence is compromised and the scientific exchange defense for their activities weakens. While no single statute mandates the specific organizational structure, FDA guidance on off-label promotion and the OIG compliance framework together create strong regulatory expectations that MSL functions operate independently of commercial direction. Industry consensus and best practice reinforce this as a structural requirement, not merely an internal preference.
Strategic: The MSL's commercial value depends on KOLs, thought leaders, and evidence-based prescribers believing they are receiving genuine scientific engagement rather than a more sophisticated form of promotion. This credibility drives three commercially relevant outcomes: KOL scientific advocacy that influences peer prescribing, clinical objection handling that prevents HCP drop-off during the prescribing decision, and health system access through formulary influence that commercial reps can't directly deliver. All three disappear if KOLs perceive the MSL as a commercial agent.
The independence that creates the compliance requirement is also what generates the commercial value. The constraint and the asset are the same thing.
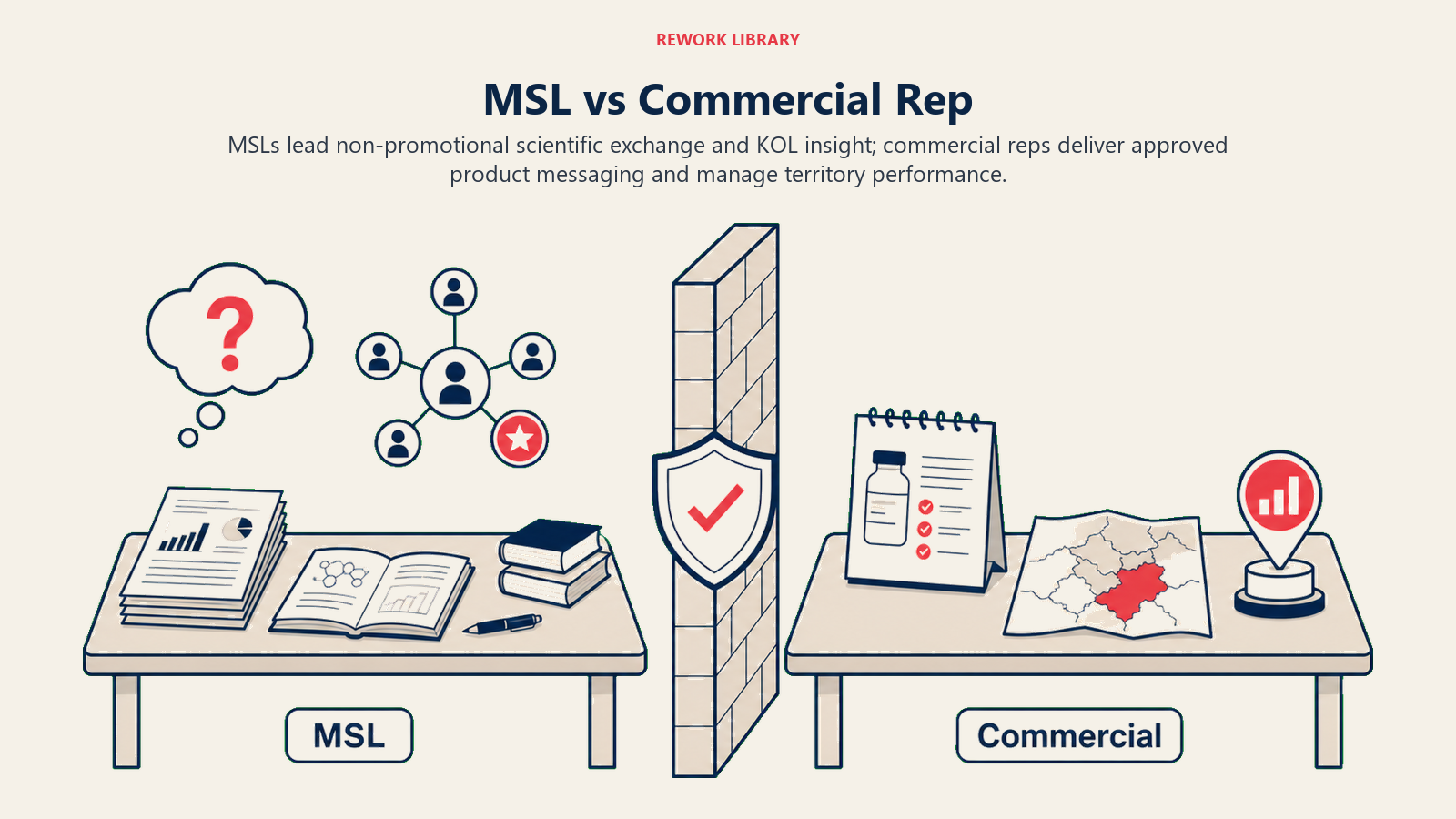
MSL vs. Commercial Rep: Role Comparison
Understanding the boundary between these roles is the foundation of an effective coordination model.
| Dimension | Medical Science Liaison | Medical Representative |
|---|---|---|
| Organizational home | Medical affairs | Commercial / sales |
| Primary objective | Scientific exchange, evidence generation support, clinical education | Prescription demand generation, territory growth |
| Customer interactions | KOLs, thought leaders, research investigators, pharmacy and therapeutics (P&T) committee members, formulary decision-makers | Prescribers (GPs, specialists), pharmacists (via pharmacy reps) |
| Content authorized to discuss | Approved and unapproved (upon unsolicited request) clinical data, mechanism of action, disease education, real-world evidence | Approved promotional content only, within labeled indication |
| Incentives | Activity-based (calls, KOL engagements, publications supported); NOT tied to sales metrics | Script volume, territory growth, call frequency |
| Training | Clinical/scientific background (PharmD, PhD, MD typical) | Product training, sales methodology |
| Reporting | VP Medical Affairs or Chief Medical Officer | Sales director / commercial leadership |
| Regulatory classification | Non-promotional (when conducted correctly) | Promotional |
This table isn't an organizational preference. It's a description of what regulators expect and what KOLs require for the MSL function to retain its credibility.
The Collaboration Paradox: MSLs Cannot Promote, But Their Work Drives Prescriptions
Here's the apparent contradiction that makes medical-commercial alignment so difficult to navigate: MSLs are explicitly prohibited from promotional activities, but their work is one of the most commercially valuable investments a pharma company can make.
KOL credibility translates to prescribing influence. A KOL who believes in a product's science based on independent evaluation of the clinical evidence, facilitated by honest MSL engagement, influences their peer community in ways that no promotional campaign can replicate. Peer-to-peer recommendation at conferences, in journal commentary, and in hospital department meetings drives prescribing behavior among the HCPs those KOLs influence. The MSL doesn't generate that peer influence directly. But the MSL's scientific engagement is what creates the informed, credible KOL who generates it.
Clinical query handling prevents prescriber drop-off. Complex therapy areas involve prescribers who want scientific answers before committing to a prescribing decision. A rep isn't authorized to answer a question about investigational data or off-label use. If the rep escalates to a medical information hotline, the response is typically delayed and impersonal. If the MSL can follow up directly with the clinical context the prescriber needs, the prescribing decision doesn't stall. This prevention of prescriber drop-off has direct commercial value even though the MSL interaction itself is not promotional.
Medical education events generate prescriber pipeline. MSL-facilitated medical education events, symposia, and advisory boards bring prescribers into scientifically credible contact with clinical evidence about a product in a context that's not promotional. The prescribers who attend these events and engage with the data are more likely to consider the product when it's relevant to their patients. Commercial reps benefit from this prescriber education even though they didn't create it.
The commercial value is real. The mechanism is indirect. And the indirect mechanism is precisely what must be protected.
Alignment Without Contamination: Where MSL and Commercial Can Coordinate
The challenge for pharma leaders is not choosing between medical affairs independence and commercial performance. It's designing a coordination model that enables both. The Firewall-with-Doors Model structures this: the firewall between medical and commercial is kept strong enough that KOLs trust the MSL function as genuinely independent, while specific coordination doors are designed within that firewall for the information flows that are both compliant and commercially valuable. Four legitimate coordination areas sit inside those doors; everything else stays outside. There are specific, well-defined areas where MSL and commercial can legitimately coordinate, and specific areas where they cannot.
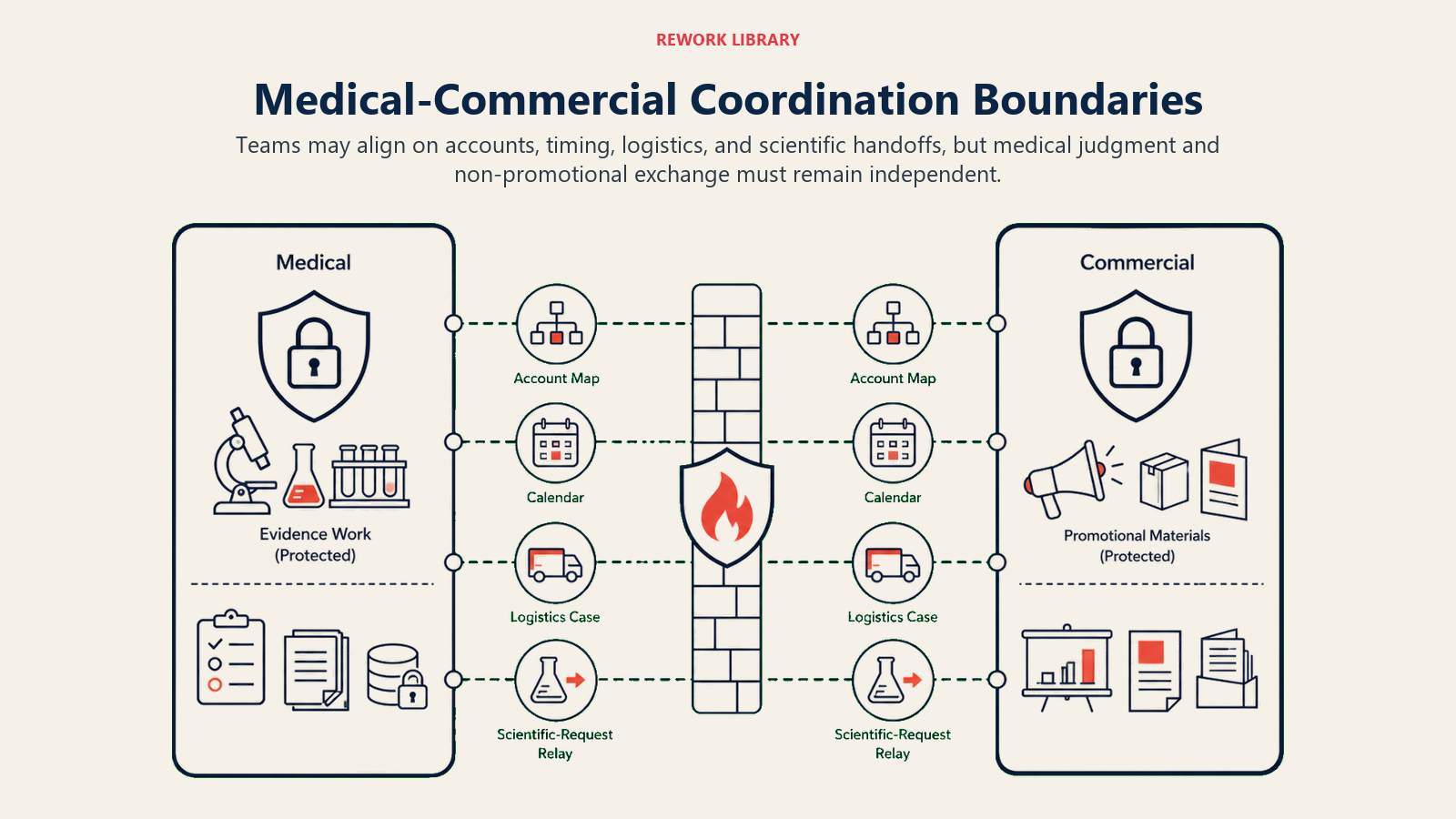
Legitimate Coordination Area 1: Territory and Account Planning
MSLs and medical representatives can and should align on account universe mapping: identifying which HCPs and health systems matter most for the product, which are KOLs with genuine peer influence, and which have barriers to prescribing that have a scientific rather than commercial root.
The coordination mechanism is a shared account list with separate call objectives. The MSL and the rep may both have the same cardiologist in their priority account list. The rep's call objective is a detailing conversation focused on approved promotional content. The MSL's call objective is scientific exchange on real-world evidence in heart failure patients. These objectives are documented separately and must not contaminate each other.
What's allowed: shared account prioritization based on clinical influence and commercial importance. What's not allowed: the commercial team directing the MSL on call frequency to specific accounts based on prescribing targets.
Legitimate Coordination Area 2: Scientific Objection Hand-Off
When a medical representative encounters a clinical question they're not authorized to answer in a detailing call, whether that's a question about investigational data, a request for comparative safety detail beyond the approved label, or a complex pharmacoeconomic question, the correct response is to flag the question and initiate an MSL follow-up.
This hand-off protocol is both compliant and commercially valuable. It prevents the rep from attempting an answer that could create regulatory exposure. It gives the prescriber a credible scientific response that addresses their actual concern. And it creates an MSL contact point with a prescriber who already has some product familiarity from the commercial interaction.
The hand-off must be genuinely unsolicited from the MSL's perspective. The MSL follows up because a healthcare professional has a scientific question, not because a commercial rep has identified a potential prescribing convert and wants scientific reinforcement.
Legitimate Coordination Area 3: KOL Intelligence Sharing (One Direction Only)
MSLs develop deep knowledge of the KOL landscape in their territory: who the genuine thought leaders are, what clinical questions they're focused on, what data gaps they've identified, what their peer relationships look like. This intelligence is commercially valuable for targeting, prioritization, and campaign strategy.
The permitted flow is MSL to commercial: intelligence about KOL scientific priorities and clinical interests informs commercial targeting and HCP segmentation. The blocked flow is commercial to MSL: commercial teams must not direct MSL call activity, messaging, or content based on sales objectives.
The one-way nature of this information flow isn't bureaucratic caution. It's the mechanism that keeps the MSL's scientific credibility intact. If KOLs learn that MSL visit patterns are driven by commercial targeting decisions rather than scientific relevance, the MSL-KOL relationship becomes promotional by implication.
Legitimate Coordination Area 4: Medical Education Events
Medical education events represent one of the most effective points of medical-commercial coordination when they're structured correctly.
The MSL designs and runs the scientific content: the clinical presentation, the evidence review, the case study discussion. The commercial team handles event logistics: venue booking, invitations to target prescribers, post-event follow-up for prescribers who have clinical questions that can be directed to the rep.
The boundary: the MSL must not be in the room when commercial follow-up is discussed, and the scientific content of the event must not be designed to drive a specific prescribing behavior. The education is genuinely educational. The commercial benefit comes from prescribers having accurate, credible clinical information that allows them to make informed prescribing decisions.
What Is Off-Limits: Compliance Boundaries in Plain Language
The following activities represent compliance violations that can expose a pharma company to regulatory enforcement, off-label promotion allegations, and breakdown of the scientific credibility that makes MSLs effective. The OIG Compliance Program Guidance for Pharmaceutical Manufacturers identifies manufacturer compensation relationships with physicians connected to marketing and sales activities as a documented fraud and abuse risk area.
MSL cannot: attend sales team meetings where prescribing targets or promotional strategy are discussed; receive compensation or performance assessments tied to territory sales metrics; take direction from commercial leadership on call content, message emphasis, or target prioritization; use KOL relationships to deliver what is effectively promotional messaging under a scientific cover.
Commercial cannot: direct MSL call activity based on prescribing targets or territory performance needs; share MSL call reports with the sales team for territory planning purposes; represent to HCPs that MSL engagement is anything other than independent scientific exchange; expect or pressure the MSL to advance promotional objectives in scientific conversations.
These boundaries aren't optional. But they also don't prevent meaningful coordination. The companies that handle this well have internalized the boundaries so thoroughly that they rarely come up as friction. The coordination model is designed around the firewall, not despite it. The PhRMA Code on Interactions with Health Care Professionals provides the industry standard framework underpinning these separation requirements.
See pharmaceutical marketing compliance and ethics for the regulatory framework underpinning these boundaries.
Governance and Firewall Design: The Medical-Commercial Interface Committee
Sustainable medical-commercial alignment requires a governance structure that makes the boundaries explicit, provides a formal mechanism for coordination within those boundaries, and creates an escalation path when the lines are at risk of being crossed.

Medical-Commercial Interface Committee: Recommended Structure
| Component | Detail |
|---|---|
| Chair | Head of Medical Affairs (not commercial, to preserve medical independence in governance) |
| Members | VP Commercial, MSL director, field sales director, compliance officer, legal representative |
| Frequency | Monthly operational meeting; quarterly strategic review |
| Agenda items | KOL landscape intelligence sharing (MSL to commercial); hand-off protocol review; medical education event planning; escalation of boundary disputes; upcoming data releases and scientific milestones that commercial needs to prepare for |
| What is NOT on the agenda | Sales targets, rep performance by territory, promotional campaign messaging, MSL call frequency objectives |
The committee design reflects the principle that the firewall has doors. The monthly meeting is a door: a structured, documented, compliance-supervised mechanism for the information flows that are legitimate and commercially valuable. The compliance officer's presence at every meeting is not there to slow things down. It's there to make the door trustworthy so it stays open. Applying RACI discipline to commercial operations produces a similar benefit in other industries: when ownership is explicit and documented, escalation paths are clear and coordination becomes routine rather than contentious.
Escalation path: when a commercial team member asks for something that approaches a compliance boundary (asking MSLs to prioritize visits to top prescribers, requesting MSL call reports for territory planning, asking MSLs to reinforce a specific promotional message), the escalation goes to the compliance officer and the head of medical affairs, not to commercial leadership. The independence of that escalation path is what makes the governance credible.
Scientific Objection Hand-Off Protocol
The most operationally critical interface between MSL and commercial is the scientific objection hand-off. Here's a practical protocol:
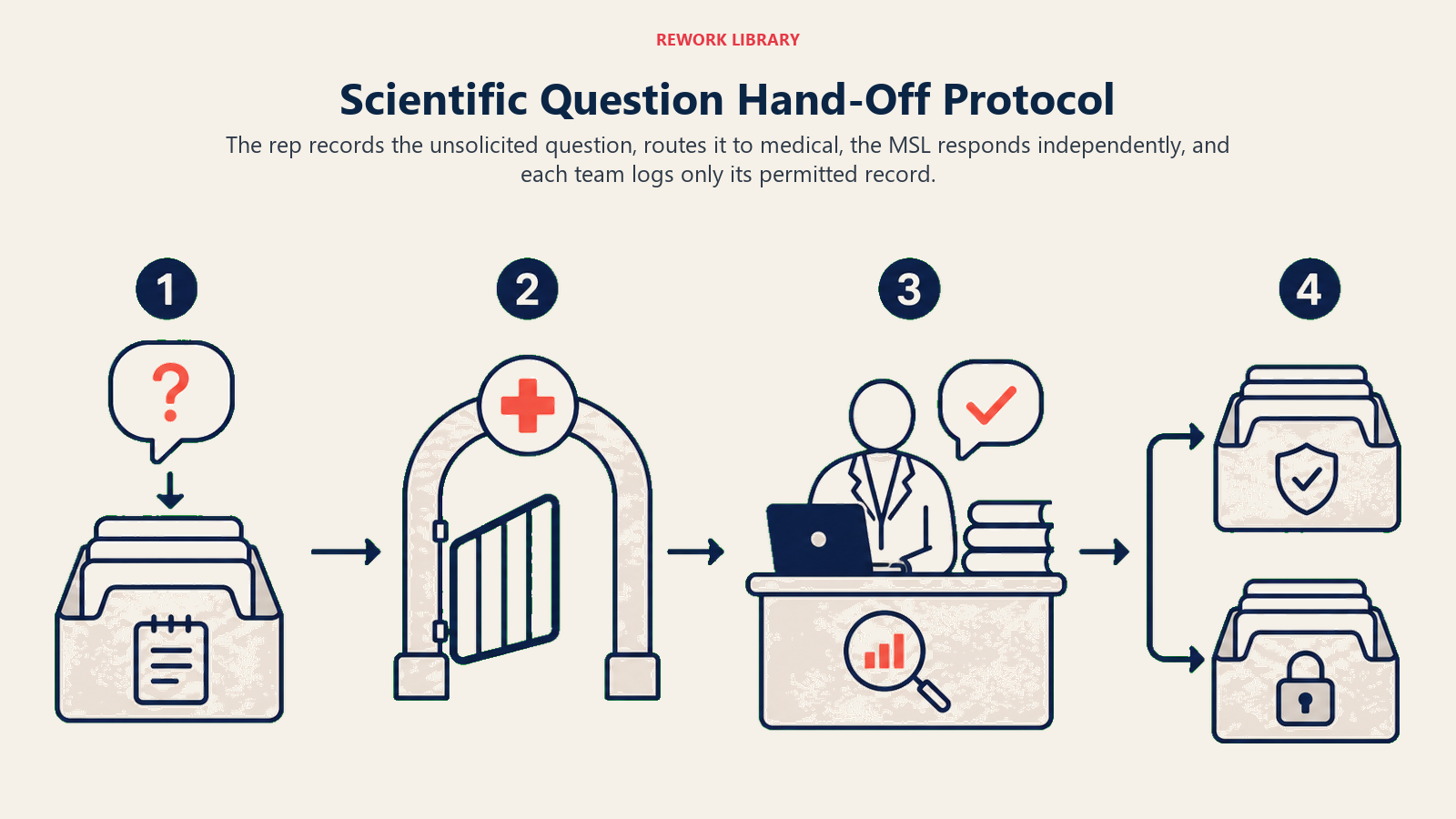
Step 1: Rep encounters a clinical question in a detailing call that exceeds approved promotional content. Rep acknowledges the question and commits to facilitating a scientific follow-up.
Step 2: Rep enters the question in the CRM under a "scientific inquiry" category (separate from promotional call notes). The entry captures only the nature of the question, the HCP's contact information, and the preferred contact time. It does not capture prescribing data or commercial context.
Step 3: MSL receives the hand-off notification through a system accessible to medical affairs. MSL reviews and schedules follow-up independently, based on their own assessment of the scientific relevance.
Step 4: MSL follows up with the HCP with no commercial context provided by the commercial team and no expectation of a prescribing outcome from the interaction.
Step 5: If the MSL conversation generates a further clinical question relevant to the rep's next visit, the MSL may communicate the general nature of the HCP's scientific interest (not a prescription intent signal) to the rep, through the same formalized channel.
This protocol is not administratively burdensome. It's two data entry steps and a documented hand-off. The documentation protects the company. The independence of the MSL follow-up protects the relationship.
KOL Intelligence: The One-Way Feed That Makes Alignment Work
The KOL landscape is the highest-value intersection of medical and commercial work. KOL identification and recruitment works when it's treated as a medical-generated asset that commercial benefits from, not a commercial-directed priority that MSLs execute on. The most scientifically credible thought leader for your product is not necessarily the highest-volume prescriber: chasing volume over scientific fit produces relationships that carry neither commercial weight nor scientific credibility. The same lesson applies to customer segmentation and targeting more broadly: the accounts that look biggest are not always the ones where influence actually flows.
When MSLs identify KOLs based on scientific criteria and share that intelligence through the governance process, the KOL relationship is real and the peer influence is genuine. When commercial directs MSL prioritization based on prescribing targets, MSLs end up in relationships with high-volume physicians who have limited scientific credibility, and the advocacy that results carries no peer weight.
For how prescription demand generation connects to MSL-facilitated scientific education, see the Prescription Demand Generation article in Learn More.
Conclusion: The Firewall Has Doors
The medical-commercial boundary in pharma isn't an obstacle to commercial performance. When it's designed and governed properly, it's a commercial advantage.
The companies that perform best in therapy areas requiring complex clinical engagement aren't the ones that blur the medical-commercial line. They're the ones that have invested in making the firewall strong enough that KOLs and HCPs trust the MSL function as genuinely independent, and then designed collaboration doors within that firewall that let commercial teams benefit from the credibility the MSL function builds.
Strong firewall, well-designed doors. That's the model.
A KOL who trusts an MSL because that MSL has never done anything promotional will speak differently about a product than one who has learned to see every scientific interaction through a commercial lens. The prescribing community in any specialty is small. That trust, or its absence, spreads.
Alignment is not about eliminating the boundary between medical and commercial. It's about managing the boundary so deliberately that the commercial team captures every legitimate benefit of MSL work without ever compromising the independence that makes that work valuable.
The alternative, letting the boundary erode for short-term commercial convenience, trades the most credible scientific asset in the field force for an incremental promotional interaction. That's a bad trade every time.
Frequently Asked Questions about Medical MSL and Commercial Alignment
What is a Medical Science Liaison and how do they differ from a medical rep?
An MSL is a field-based scientific expert employed in the medical affairs function who engages KOLs, research investigators, and health system decision-makers on clinical content beyond what a promotional rep can discuss. Unlike medical reps, MSLs are not measured on sales metrics, do not carry promotional materials, and can discuss investigational data and real-world evidence when requested by healthcare professionals. Their credibility depends on demonstrating genuine scientific independence from commercial objectives.
Why must MSLs report to medical affairs rather than commercial?
FDA regulations distinguish between promotional activities, which must be consistent with the approved label, and scientific exchange, which can cover broader scientific context. If MSLs report to commercial leadership, receive sales-based incentives, or take direction from commercial teams on call content, that independence is compromised and the scientific exchange defense for their activities weakens. While no single statute mandates a specific org-chart structure, FDA guidance on off-label promotion and OIG compliance expectations together create strong regulatory pressure for MSLs to sit outside commercial. Industry consensus treats this as a structural best practice, and departing from it carries material regulatory and reputational risk.
What commercial value do MSLs generate without promoting?
MSLs generate commercial value through three indirect mechanisms. First, KOL peer advocacy: a scientifically credible KOL who believes in a product based on honest MSL engagement influences peer prescribing at conferences, in journal commentary, and in hospital department meetings in ways no promotional campaign can replicate. Second, clinical query handling that prevents prescriber drop-off when a rep cannot answer a complex scientific question. Third, formulary and health system access through P&T committee relationships that commercial reps cannot directly cultivate.
What are the four legitimate areas where MSL and commercial can coordinate?
The four compliant coordination areas are: shared account prioritization (same account list with separate objectives), scientific objection hand-off (rep flags a clinical question, MSL follows up independently), one-directional KOL intelligence sharing from MSL to commercial, and medical education event collaboration where the MSL runs scientific content and commercial handles logistics. All four require documented governance and a compliance officer present at coordination meetings.
What specific activities are off-limits for MSLs and commercial teams?
MSLs cannot attend meetings where prescribing targets or promotional strategy are discussed, receive performance assessments tied to territory sales metrics, or take commercial direction on call content or target prioritization. Commercial teams cannot direct MSL call activity based on prescribing targets, share MSL call reports with the sales team for territory planning, or expect MSLs to reinforce promotional objectives in scientific conversations. These are not guidelines but requirements, and violations can trigger OIG enforcement and erode KOL trust.
How does the scientific objection hand-off protocol work?
When a rep encounters a clinical question beyond the approved promotional scope, they acknowledge it and commit to facilitating scientific follow-up. The rep enters the nature of the question in the CRM under a scientific inquiry category, capturing only the question type and HCP contact information, not prescribing data or commercial context. The MSL receives the hand-off through a medical affairs system, reviews it independently, and follows up with no commercial context and no expectation of a prescribing outcome. This two-step protocol protects both the company and the KOL relationship.
Why does KOL intelligence flow only from MSL to commercial and not the reverse?
If commercial teams direct MSL visit patterns based on prescribing volume, MSLs end up in relationships with high-volume physicians who may have limited scientific credibility. The advocacy generated from those relationships carries no peer weight in the prescribing community. KOL selection based on scientific criteria produces relationships where peer endorsement is genuine and spreads through networks of clinically influential peers. The one-way information flow is what keeps KOL credibility from becoming a commercial commodity.
Learn More

Senior Implementation Consultant
On this page
- What MSLs Do and Why They Sit in Medical, Not Commercial
- MSL vs. Commercial Rep: Role Comparison
- The Collaboration Paradox: MSLs Cannot Promote, But Their Work Drives Prescriptions
- Alignment Without Contamination: Where MSL and Commercial Can Coordinate
- Legitimate Coordination Area 1: Territory and Account Planning
- Legitimate Coordination Area 2: Scientific Objection Hand-Off
- Legitimate Coordination Area 3: KOL Intelligence Sharing (One Direction Only)
- Legitimate Coordination Area 4: Medical Education Events
- What Is Off-Limits: Compliance Boundaries in Plain Language
- Governance and Firewall Design: The Medical-Commercial Interface Committee
- Scientific Objection Hand-Off Protocol
- KOL Intelligence: The One-Way Feed That Makes Alignment Work
- Conclusion: The Firewall Has Doors
- Learn More