Independent vs Chain Pharmacy Strategy: How Pharma Companies Win Both Channels
Turn this article into takeaways for your work.
Each assistant summarizes the article only for you and suggests best practices for your work.
Send the same sales pitch to a family-owned pharmacy on a high street and to the category manager of a 300-store pharmacy chain, and you'll fail at both. One wants to know whether the product is worth recommending to the retired patients who trust her recommendations. The other wants to know what your shelf placement fee looks like and whether your promotional calendar aligns with her Q3 category review.
Same product. Completely different conversations.
Most pharma companies know this conceptually but still run a single pharmacy channel strategy that half-heartedly attempts both. The territory manager visits the independent pharmacist on Tuesday and the chain key account on Thursday with essentially the same presentation and the same trade terms. The independent pharmacist feels underserved by someone who clearly doesn't understand her business. The chain category manager wonders why this company is sending a territory rep to a negotiation that belongs in a head-office commercial meeting.
The pharma companies that win pharmacy consistently are the ones that treat these as genuinely different businesses requiring different people, different processes, and different commercial propositions.
Defining the Segments: It's Not Just Independent vs Chain
The binary "independent vs chain" framing is a useful starting point, but the reality is more granular. The pharmacy universe in most markets splits into at least five distinct segments, each with different buying dynamics.

Independent pharmacists own and operate single-outlet or small multi-outlet businesses. The owner is typically the pharmacist, the buyer, the recommender, and the P&L accountable person. Decisions are made at the counter and completed in the same conversation. Margin, product availability, clinical credibility, and personal relationship all influence whether they stock and recommend your brand. In most emerging markets, independent pharmacies represent the large majority of outlets by count, often estimated at 70-80% or higher in markets like India, Southeast Asia, and sub-Saharan Africa, though their share of total prescription volume is declining as organized retail grows. These are market-specific estimates; coverage varies widely by country and urbanization level. In the United States, independent pharmacies account for nearly 36% of all retail pharmacies, with no single chain operating more locations than all independents combined.
Regional chains operate 10-100 outlets under common ownership, often concentrated in a single city or state. They have more formal buying processes than independents but are typically still owner-managed or family-operated. The buying decision often sits with a commercial director or purchasing manager rather than individual store owners, but relationship and local presence still matter.
National chains operate hundreds to thousands of outlets through professional management structures with centralized category management, planogram enforcement, and annual promotional calendars. In markets where national chains have emerged (Southeast Asia, parts of Africa, the Gulf), they require a full key account management approach: negotiations happen at the head office level, terms are national, and execution is monitored through periodic range reviews.
Hospital-linked retail pharmacies operate within or adjacent to hospital campuses. They carry a skewed portfolio tilted toward the hospital's formulary, serve patients being discharged or attending outpatient clinics, and often have procurement linked to the hospital's central pharmacy. These accounts require hospital formulary inclusion before retail listing becomes commercially meaningful.
E-pharmacies have grown significantly in markets where digital health infrastructure and regulatory frameworks support online prescription fulfillment. In markets where public health insurance systems are expanding, e-pharmacies and organized retail chains are increasingly being contracted into public supply chains, a trend documented in research on pharmacy access reforms in low- and middle-income countries, where geographic equity and stock reliability are the central design challenges in public-sector pharmacy contracting. The buying model is platform-based (SKU listing, digital shelf placement, search ranking) rather than relationship-based, and the commercial conversation happens with a category or operations manager at the platform level, not at an outlet.
Key Facts: Independent vs Chain Pharmacy Strategy
- Independent pharmacies account for nearly 36% of all retail pharmacies in the United States, with no single chain operating more locations than all independents combined (NCPA 2025 Digest Report).
- For OTC (over-the-counter) and pharmacy-only products, the pharmacist's recommendation is the dominant driver of consumer choice. In independent pharmacies, winning the pharmacist's recommendation wins the sale (PMC6861682).
- Research on pharmacy access reforms in low- and middle-income countries documents the shift toward contracting retail pharmacies into public supply chains, where geographic equity and stock reliability are the central design challenges in public-sector pharmacy systems (PMC10153779), context relevant to pharma companies operating in markets where government health insurance is expanding into retail pharmacy channels.
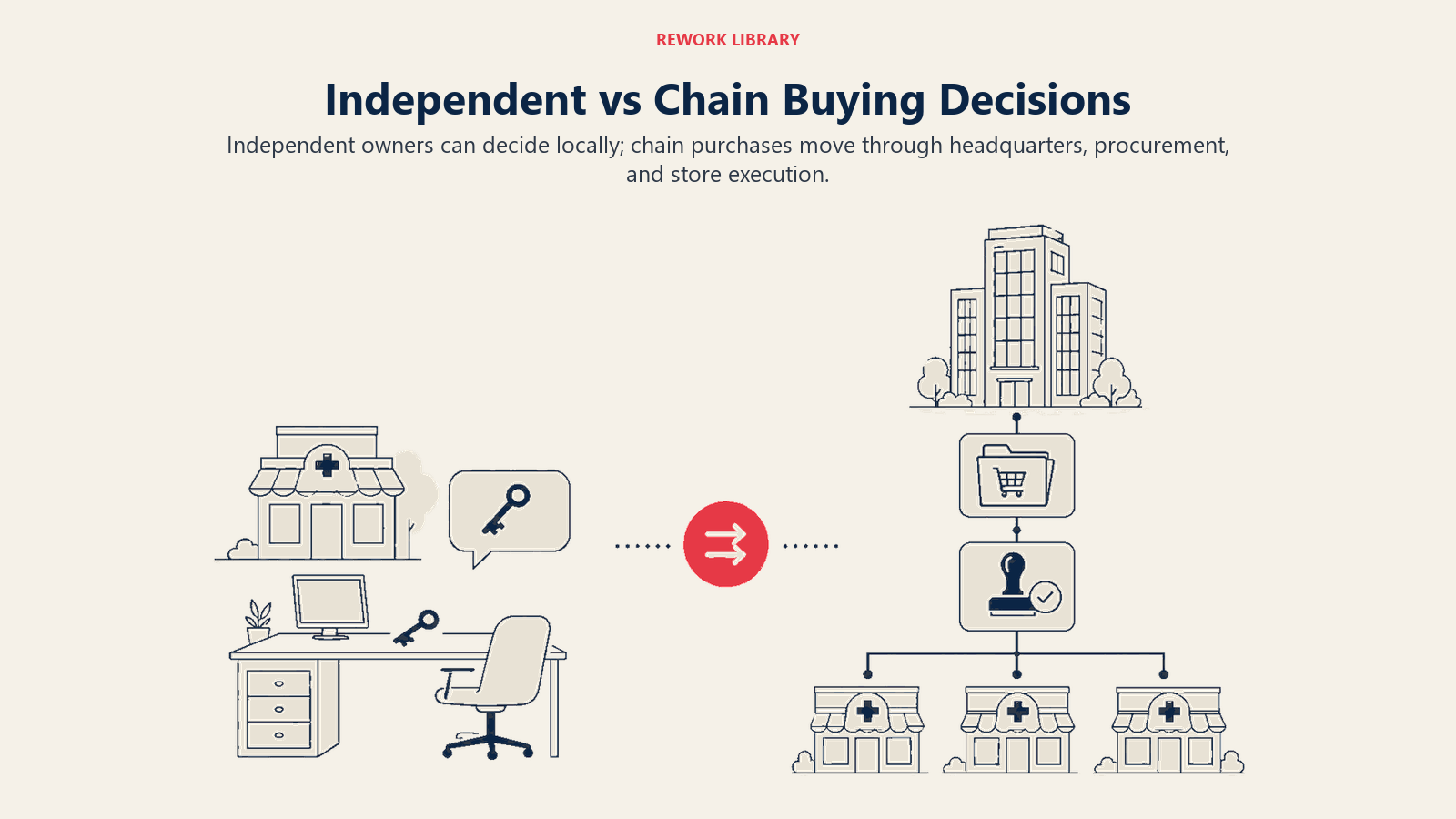
Decision-Making Differences: Who Buys, Who Recommends, Who Matters
The single biggest mistake pharma companies make in pharmacy channel management is targeting the wrong person. The decision-maker varies by segment and by what you're trying to achieve: stocking the product versus recommending the product versus displaying it prominently versus running a promotional campaign.
| Pharmacy Segment | Stocking Decision | Recommendation Influence | Promotional Agreement | Data You Can Get |
|---|---|---|---|---|
| Independent | Owner-pharmacist | Owner-pharmacist | Owner-pharmacist | Manual tracking only |
| Regional chain | Commercial director / buyer | Store pharmacists | Commercial director | Partial (store-level or aggregate) |
| National chain | Category manager (HQ) | Store pharmacists | Category manager (HQ) | POS data (negotiated) |
| Hospital-linked | Pharmacy committee / procurement | Clinical pharmacist | Procurement manager | Internal usage data |
| E-pharmacy | Category / operations manager | Algorithm + reviews | Category manager | Digital analytics |
For prescription products, this distinction matters enormously. The category manager at a national chain can decide to list your product across 300 stores, but she can't make pharmacists recommend it over a competing brand. You still need pharmacist-level clinical education and relationship investment to drive recommendation behavior. Listing and recommendation are separate commercial outcomes requiring separate commercial strategies.
For OTC and pharmacy-only products, the pharmacist's recommendation power is the dominant driver of consumer choice. In independent pharmacies, winning the pharmacist's recommendation wins the sale. In chain pharmacies, you need both: HQ agreement on listing and range, and pharmacist-level engagement to drive recommendation at the counter.
Independent Pharmacy Strategy: Relationship, Education, Loyalty
Independent pharmacists don't respond well to transactional selling. They're healthcare professionals who take their recommendation responsibility seriously, and they're business owners who make margin and turnover calculations for every product they stock. Your commercial approach needs to address both dimensions.
Relationship-led selling: The territory rep visiting an independent pharmacist is, in most markets, the most frequent point of contact between the pharma company and that pharmacy. The quality of that relationship determines whether the pharmacist stocks your brand, recommends it when a patient presents, and re-orders proactively when stock runs low. Reps working independent pharmacies need genuine pharmacist engagement skills, not just a call script. They need to know the pharmacist's patient population, understand which therapeutic areas she's most active in, and bring clinical information that's relevant to her practice.
Clinical education: Independent pharmacists respond to product knowledge delivered in clinical terms. What's the mechanism of action? What's the evidence base? Which patient profile benefits most? What drug interactions should she flag? A rep who can have that conversation has immediate credibility differentiation over one who leads with price and margin.
Loyalty programs: Tiered loyalty schemes that reward cumulative purchase volume, clinical training completion, or referral activity are effective in independent pharmacy channels where the owner-pharmacist is both the buyer and the beneficiary. See Pharmacy Loyalty and Incentive Programs for program design principles. The key is designing rewards that reinforce stocking and recommendation behavior rather than simply subsidizing price.
Credit terms: Many independent pharmacies in emerging markets operate on thin working capital and rely on distributor credit to manage cash flow. Where your products move through distributors who extend credit to pharmacies, the effective credit term is part of your commercial proposition even if you don't directly control it. Some pharma companies negotiate extended credit windows with their distributors as part of the channel incentive structure.
Visit frequency and call focus: Independent pharmacy visits should balance relationship maintenance, stock check and re-order facilitation, and clinical education. The optimal call frequency for independent pharmacies depends on the therapeutic category (higher-frequency chronic care products justify more frequent visits than acute care products) and the outlet's prescription volume potential. A monthly visit cycle is typical for tier-1 independent pharmacies; quarterly for tier-2. The visit structure should be consistent enough that the pharmacist expects and prepares for the rep's call, not so scripted that it feels like a checklist.
The chain pharmacy conversation operates on an entirely different calendar and requires an entirely different room.
Chain Pharmacy Strategy: Key Accounts, Agreements, and Data
Chain pharmacies require a completely different commercial model. The buying decision is institutional, not personal. The timeline is annual or semi-annual (aligned to category review cycles), not visit-by-visit. And the commercial levers are shelf placement, promotional support, and data sharing, not relationship and clinical education.
Key account management: National and large regional chains should be managed by dedicated key account managers (KAMs), not by territory reps. A KAM working a national chain account is negotiating annual trading terms, co-promotional investments, and data-sharing agreements. This is a different skill set from territory selling: it requires financial modeling, negotiation discipline, and the ability to present a category growth story rather than a product story.
Shelf placement agreements: Chain pharmacies control which products appear on the shelf, where, and in what display format. A shelf placement agreement might specify a minimum number of facings, a planogram position (eye level, counter display, specific shelf bay), and a price band compliance commitment. Placement agreements are typically part of annual trading term negotiations and may be linked to a co-investment from the manufacturer in the form of a listing fee, a category management contribution, or co-funded promotional activity.
Promotional calendars: Chains plan promotions months in advance, typically through a category manager or trade marketing function. To participate in a chain's promotional program, you need to be in their planning cycle early, which means understanding their promotional calendar format, submission timelines, and the commercial requirements for promotional participation. A pharma company that shows up asking for a promotion inclusion after the calendar is locked will get nothing, or an expensive late-addition placement that didn't benefit from the chain's full promotional support.
Co-op marketing: Many large chains offer co-funded marketing programs: in-store communications (aisle markers, counter cards, staff recommendation programs), digital marketing (email campaigns to registered customers, app push notifications), and loyalty program integration (purchase points on your brand). These programs can drive meaningful incremental offtake but require a structured investment proposal and clear measurement of uplift.
Data sharing: The most valuable commercial relationship you can build with a national chain pharmacy is one where they share point-of-sale (POS) offtake data. Chain pharmacy POS data is tertiary sales visibility at its most granular: you can see exactly which stores, in which cities, are selling your product at what rate, how your sales compare to the category benchmark, and where your share is losing to competitors. Use this data to optimize your field force deployment and your promotional investment allocation. Not all chains will share POS data freely; some charge for it, others include it as part of a trading terms discussion, and a few treat it as proprietary. The question of how to split resources between the two channel types starts from the same data.
How Should Pharma Companies Allocate Resources Across Pharmacy Channel Types?
The central resource allocation question in pharmacy channel management is how to divide rep time, KAM headcount, and trade marketing budget across the two channel types. There's no universal answer, but the framework is straightforward. The Dual-Track Coverage Model provides the structure: independent pharmacies are managed through relationship-led territory reps using clinical education, loyalty programs, and distributor credit as the primary commercial levers; chain pharmacies are managed through KAMs at the headquarters level using shelf placement agreements, promotional calendars, and POS data-sharing as the primary commercial levers. The two tracks run in parallel, with separate measurement systems, separate commercial terms, and a shared outcome metric of retail offtake by channel segment.
Start with volume concentration: In most markets, a small share of pharmacy outlets, typically the top 20-30% by prescription volume, generates the majority of commercial throughput. Map your outlet universe by estimated potential and decide which outlets belong in which tier. The exact concentration varies by market and category; use your own secondary-sales data or distributor route reports to establish the actual split in your territory. Tier-1 accounts (typically high-volume independents, all key chain accounts) get the highest engagement; tier-3 accounts might receive only distributor-led coverage. This tiering logic is the same principle that drives pharma field force territory design: segment by value potential, assign the right coverage model to each tier, and resist the temptation to give high-touch resources to accounts that won't generate a proportionate return. See Customer Segmentation and Targeting for how this plays out at the prescriber level in pharma territories.
Match resource type to segment: Independent pharmacy coverage belongs to territory reps or pharmacy relationship managers. Chain pharmacy management belongs to KAMs with headquarters-level commercial authority. Sending a territory rep to negotiate with a chain category manager is a mismatch that usually produces poor outcomes for both sides. The underlying principle is that different buyer types require different selling motions, which is exactly what Sales Methodologies Compared maps out: a relationship-led consultative approach fits the independent pharmacist, while a value-based commercial framework fits the chain category manager reviewing an annual promotional calendar.
Trade marketing budget allocation: The right split between chain and independent pharmacy programs depends on where your volume concentration lies and your strategic growth priorities. In markets where both segments are significant, a starting point of roughly half the budget toward each is reasonable, but companies in markets with rapidly growing chain pharmacy sectors may direct 60-70% to chain programs, while those in markets where independents still dominate prescription volume will rebalance the other way. Adjust based on actual offtake data, not a preset ratio.
Suggested Coverage Model
| Segment | Account Management | Visit Frequency | Trade Investment | Data Return |
|---|---|---|---|---|
| National chains | Dedicated KAM (HQ) | Monthly (commercial) | High (listing, promos, co-op) | POS data (negotiated) |
| Regional chains | KAM or senior territory | Monthly (commercial) | Medium | Aggregate store data |
| Tier-1 independent | Territory rep | Monthly | Low-medium (loyalty, credit) | Manual tracking |
| Tier-2 independent | Territory rep | Quarterly | Low (loyalty tier) | Manual spot-check |
| Tier-3 independent | Distributor-led only | As covered by van sales | Minimal | None reliable |
Measurement and Tracking: Making the Two Segments Comparable
The asymmetry between chain and independent pharmacy data creates a reporting challenge. Chain pharmacies (if you've secured data sharing agreements) give you granular POS offtake by store and SKU. Independent pharmacies give you virtually nothing unless your field reps are conducting systematic stock checks during visits.
The practical solution is a two-track measurement approach that uses different proxies for the same underlying metric (retail offtake) depending on what data is available.
For chain pharmacies: POS data tracks actual offtake. Supplement with rep-reported observations during store visits (shelf position, compliance with planogram, availability of promotional materials).
For independent pharmacies: Use distributor secondary-sales data to estimate segment offtake, and use rep-reported stock-on-hand data from pharmacy visits as a proxy for how quickly product is moving. A pharmacy that consistently holds one to two weeks of stock on hand is moving product. One that holds three months of stock but doesn't re-order is a warning sign.
Common measurement framework: Report both channels against the same KPIs (offtake growth rate, brand share in category, stock availability) even though the data sources and precision levels differ. This keeps commercial leadership comparing the two channels on the same dimensions rather than treating chain pharmacy performance as "real data" and independent pharmacy performance as anecdote.
Both approaches are described in more depth in the Learn More section below. The measurement gap between chain and independent pharmacies points to a broader strategic question: what happens when companies over-index on one channel because the data is cleaner?
Sending a territory rep to negotiate annual trading terms with a chain category manager is a mismatch of authority, process, and commercial language that typically produces poor outcomes for both sides. The buyer is expecting a commercial case and a data story. The rep is prepared for a relationship call.
A Portfolio Approach Builds Resilient Shelf Presence
The pharma companies that over-index on chain pharmacy because the data is clean and the commercial terms are legible discover a structural vulnerability when chain category managers de-list a brand to make room for a competitor's co-investment. The independents aren't there to absorb the volume, because the relationship investment was neglected.
The companies that over-index on independent pharmacies because the relationship model feels controllable miss the shift toward organized retail and find their brands invisible in the channels where urban middle-class patients are increasingly shopping.
A portfolio approach to pharmacy channels is deliberately harder to manage. It requires different people with different skills, different commercial terms, different data systems, and different investment profiles operating in parallel. But it produces something the single-channel approach can't: resilient shelf presence across the full range of outlets where patients can fill a prescription.
How well it holds depends on whether your distributor relationships are strong enough to reach both channel types consistently.
Frequently Asked Questions about Independent vs Chain Pharmacy Strategy
Why can't a single pharmacy strategy work for both independent and chain pharmacies?
The buying decision, the timeline, the commercial levers, and the people involved are entirely different in each segment. Independent pharmacy decisions happen at the counter in a single conversation with the owner-pharmacist. Chain pharmacy decisions happen at a head-office category review aligned to an annual or semi-annual calendar. The same pitch, the same terms, and the same representative type will fail both. Each segment needs its own commercial proposition.
What is the pharmacist's role in driving recommendation behavior at chain pharmacies?
A chain category manager can list your product across hundreds of stores, but she cannot make store pharmacists recommend it to patients. That recommendation behavior is built through pharmacist-level clinical education and relationship investment inside each store. For prescription products especially, listing and recommendation are separate commercial outcomes requiring separate engagement strategies. A pharma company that secures a chain listing without following up with field engagement inside the stores will see shelf presence without offtake.
How should trade marketing budget be split between independent and chain pharmacy channels?
There is no universal benchmark for this split, it depends on where your volume concentration lies, the maturity of organized retail in your market, and your strategic growth priorities. In markets where both segment types are commercially significant, starting with roughly equal allocation across the two channels is a reasonable baseline before adjusting based on actual offtake data. Where chain pharmacies are capturing a growing share of prescription fulfillment, shift the chain allocation up; where independents still dominate, rebalance toward them. Review the split annually against secondary-sales data, not against a preset ratio.
When should a pharma company use a KAM rather than a territory rep for a pharmacy account?
National and large regional chains should be managed by dedicated KAMs with headquarters-level commercial authority from the first negotiation. A territory rep lacks the financial modeling skills, negotiation authority, and category management knowledge to negotiate annual trading terms, shelf placement agreements, and co-promotional investments with a professional category manager. The mismatch creates poor outcomes for both sides. The threshold for KAM assignment is typically when the account has centralized buying, an annual category review calendar, and a dedicated commercial or category management contact.
How can pharma companies measure independent pharmacy performance without POS data?
Two proxy approaches work in parallel. First, use distributor secondary-sales data to estimate segment offtake for the independent pharmacy catchment in each territory. Second, use rep-reported stock-on-hand observations during pharmacy visits as a rough proxy for how quickly product is moving: a pharmacy consistently holding one to two weeks of stock on hand is actively selling; one holding three months of stock without reordering is not. Reporting both channels against the same KPIs (offtake growth rate, brand share, stock availability) keeps commercial leadership comparing on the same dimensions even when data precision differs.
What is the Dual-Track Coverage Model?
It is a named framework for running independent and chain pharmacy strategy in parallel with distinct commercial logic for each track. Independent pharmacies are managed through relationship-led territory reps using clinical education, loyalty programs, and distributor credit as the primary commercial levers. Chain pharmacies are managed through KAMs at the headquarters level using shelf placement agreements, promotional calendars, and POS data-sharing as the primary levers. The two tracks share a common outcome metric (retail offtake by channel segment) but operate with separate people, processes, and commercial terms.
Learn More

Senior Implementation Consultant
On this page
- Defining the Segments: It's Not Just Independent vs Chain
- Decision-Making Differences: Who Buys, Who Recommends, Who Matters
- Independent Pharmacy Strategy: Relationship, Education, Loyalty
- Chain Pharmacy Strategy: Key Accounts, Agreements, and Data
- How Should Pharma Companies Allocate Resources Across Pharmacy Channel Types?
- Measurement and Tracking: Making the Two Segments Comparable
- A Portfolio Approach Builds Resilient Shelf Presence
- Learn More