Pharmacy Order and Stock Management: How Reps Keep Shelves Full and Out-of-Stocks From Killing Sales

Turn this article into takeaways for your work.
Each assistant summarizes the article only for you and suggests best practices for your work.
A patient walks in with a prescription for your product. The pharmacist checks the shelf, checks the back room, and delivers the verdict: "We're out of stock. Do you want a substitute?" The patient says yes. That script is gone. Not delayed, not rescheduled. Gone.
Most field reps treat stock as someone else's problem: a distributor issue, a logistics failure, an operations matter that sits above the sales conversation. That framing is expensive. A pharmacy that stocks your product sells it. A pharmacy that runs out of stock loses the prescription permanently, sometimes to a competitor who's been actively managing their inventory position every single visit.
Stock management isn't a logistics function that happens to affect sales. It's a sales function that requires operational discipline to execute. The field rep who owns inventory as part of the pharmacy visit playbook consistently outsells the one who treats the shelf as scenery.
Who Actually Owns the Stock Problem in Pharmacy Sales?
Field reps do. The conventional model assigns inventory responsibility to distributors, supply chain teams, or pharmacy management systems. The rep's job, in this model, is detailing and relationship building. Stock is someone else's lane.
This model has a structural flaw: the distributor doesn't know when a specific pharmacy is about to run out. The supply chain team doesn't know that a particular pharmacist has been recommending your product at higher rates since your last visit. Only the rep, on the ground, has that local context.
Every stockout event carries three costs that don't appear in any distribution report. A peer-reviewed review of drug shortage impacts identifies economic, clinical, and humanistic consequences (including medication errors and patient dissatisfaction) that compound well beyond the immediate lost sale.
The first is the immediate script loss. A patient who needs a product today will accept a substitute today. That substitution often becomes a habit. Switching back requires active effort from both the patient and the prescribing doctor.
The second is pharmacist credibility damage. Pharmacists who run out of a product because a rep never managed the order are less likely to actively recommend that product. The recommendation is a learned behavior. Stockouts unlearn it.
The third is competitor encroachment. When your product is out, competitor products are in. Some pharmacies will increase competitor facing counts during your stockout period. Recovering that shelf space requires renegotiation. It's recoverable, but it costs visits and relationship capital.
Secondary sales data suggests that pharmacies where reps actively manage reorder cycles tend to experience materially fewer stockout events and higher sell-out rates than pharmacies served by reps who only manage primary (distributor-to-pharmacy) sales, though the exact differential varies by territory and product.
Key Facts: Pharmacy Stock Management
- Applying calculated safety stock and reorder thresholds cut average pharmacy inventory costs by 55% while maintaining zero stockout rates, according to a study on optimizing outpatient pharmacy inventory.
- A systematic review of medicine stockouts found that distribution barriers and weak supply chain information management are the most frequently cited root causes of pharmacy-level stock failures.
The In-Visit Stock Audit
The stock audit happens on every visit, not every other visit, not when something looks low. Every visit. It takes three to five minutes and produces the data that drives the order ask.

Shelf Count
Count the visible facing units on the shelf. Don't estimate. Count each SKU (stock keeping unit) separately if you carry multiple presentations (tablet count, pack size, flavor variant). A facing is one product unit visible from the front of the shelf, including units stacked behind it that share the same slot.
Record the count in your CRM (customer relationship management system) before leaving the pharmacy. The trend over time (three visits, six visits, twelve visits) is as important as the single-day count. A pharmacy that stocked 24 units three visits ago and now has 6 is approaching a stockout trajectory even if 6 units feels adequate today.
Back-Room Check
Always ask about back-room inventory. Never assume the shelf count represents total stock.
The ask is simple: "What do you have in the back for [product name]?" Some pharmacists will check. Some will estimate. Some will say they don't maintain back-room stock for OTC categories. Whatever the answer, record it.
Back-room stock matters for two reasons. First, it extends the real runway before a stockout. A pharmacy with 4 units on shelf and 20 in the back is not close to running out. Second, back-room product that never moves to the shelf is effectively out-of-stock from the patient's perspective. A product the patient can't see doesn't get chosen.
If back-room stock is high relative to sell-out rate, it may indicate a display or recommendation problem rather than an inventory problem. That changes the conversation from reorder to retail merchandising and shelf visibility.
Safety Stock Threshold
Every product in your portfolio should have a defined safety stock level: the minimum on-hand quantity below which a reorder is required to avoid stockout before the next delivery cycle.
Safety stock is product-specific and pharmacy-specific. A high-turnover item in a high-traffic pharmacy needs a higher safety stock than the same item in a lower-volume outlet. Research on optimizing outpatient pharmacy inventory found that applying calculated safety stock and reorder thresholds cut average inventory costs by 55% while maintaining zero stockout rates. The formula is straightforward:
Safety Stock = Daily Sell-Out Rate x Lead Time Days x Buffer Factor
Where buffer factor is typically 1.25 to 1.5, depending on distribution reliability in the territory.
At the start of territory coverage, negotiate safety stock thresholds with your distributor manager. Document them by pharmacy and product. During visits, compare current on-hand to safety stock threshold. If on-hand is below threshold, an order ask is mandatory, not optional.
Reorder Triggers and the Order Ask
Cover-Day Calculation
The cover-day calculation tells you how many days of stock a pharmacy currently holds for your product, based on its actual sell-out rate. It's the single most useful number in a stock management conversation.
Cover Days = (Units on Hand + Back-Room Units) / Daily Sell-Out Rate
Daily sell-out rate comes from your secondary sales data, from the pharmacist's dispensing records, or from your rolling estimate based on visit-to-visit stock movements. If a pharmacy had 20 units three weeks ago and has 8 units today, it sold roughly 12 units in 21 days: a daily rate of 0.57 units per day.
A pharmacy with 8 units on hand at a daily rate of 0.57 has 14 cover days. If the distribution cycle runs every 10 days, 14 cover days is comfortable. If the distribution cycle runs every 7 days but has had recent delays, 14 cover days starts to look thin. This kind of velocity thinking mirrors what B2B sales teams track as sales cycle length: in both contexts, the number of days between events is what determines whether a gap becomes a revenue problem.
Cover-day calculation template for in-visit use:
| Input | Value |
|---|---|
| Units on shelf | |
| Units in back room | |
| Total on hand | |
| Daily sell-out rate (units/day) | |
| Cover days = total / daily rate | |
| Next scheduled delivery (days) | |
| Status: Comfortable / Reorder / Urgent |
Any cover-day calculation below 1.5x the delivery cycle length triggers the order ask. Below 1.0x, it's an urgent reorder situation.
The Reorder Conversation
The reorder conversation links sell-out data to the order quantity ask. It's not a favor. It's a business case presented in the pharmacist's own terms.
"You've been selling through [product] at about [rate] per day. At that pace, you've got about [cover days] days of stock. Your next delivery is in [days], so I'd recommend placing an order today for [quantity] units. That keeps you covered through the next cycle with a comfortable buffer."
The ask is specific. "You should probably order more" is not an ask. "I'd recommend ordering 24 units today" is an ask. Specificity signals professionalism. It also makes it easy for the pharmacist to say yes without doing their own calculation.
Link the order to the pharmacist's economics where possible. Connect the repeat order and reorder systems to their gross margin per SKU: "At your standard margin on this product, 24 units represents about [margin amount] in contribution before the next delivery cycle."
Handling the "Distributor Will Deliver" Deflection
Many pharmacists, especially in independent outlets, rely on standing distributor delivery schedules rather than active ordering. When the rep raises a stock concern, the response is often: "The distributor delivers on Thursday. I'll be fine."
This deflection is not necessarily wrong, but it requires verification, not acceptance.
The follow-up question is: "Is there an open order on your account with the distributor for [product] right now, or are you expecting them to read the shelf and replenish automatically?"
Many distributors do not automatically replenish unless an order is placed. A pharmacist who assumes their standing delivery will include your product may be wrong. The rep's role is to confirm the order exists, not just that a delivery is scheduled.
If the pharmacist isn't certain, the rep can offer to call the distributor or stockist directly from the pharmacy counter to confirm or place the order. This takes two minutes and removes ambiguity. It also demonstrates commitment that earns trust for future visits.
Order Size Optimization
Order size is a balance between two failure modes: under-stocking that creates stockouts and over-stocking that ties up pharmacy cash and shelf space.
Over-stocking creates its own problems. A pharmacist who sits on a 90-day supply of your product is less receptive to new products, new SKUs, and investment in additional facing space. Excess inventory reduces the pharmacist's perception of product velocity, even when real sell-out is healthy.
The target order quantity is:
Recommended Order = (Daily Sell-Out Rate x Cycle Days x 1.25) minus Current On-Hand
Round up to the nearest standard pack size. The 1.25 multiplier accounts for a 25 percent demand buffer. Adjust upward if there are seasonal demand patterns (cold and flu season for relevant categories) or known promotional activity that will lift pull-through.
For pharmacies with highly variable sell-out rates (week-to-week variation greater than 30 percent), use a four-week moving average for the daily sell-out calculation rather than a recent two-week snapshot. This smooths noise and prevents dramatic swings in order quantity. The next question is whether that order gets placed by the right person at all.
Independent Pharmacy vs. Chain Pharmacy Ordering Dynamics
The ordering process differs meaningfully between independent and chain pharmacy environments.
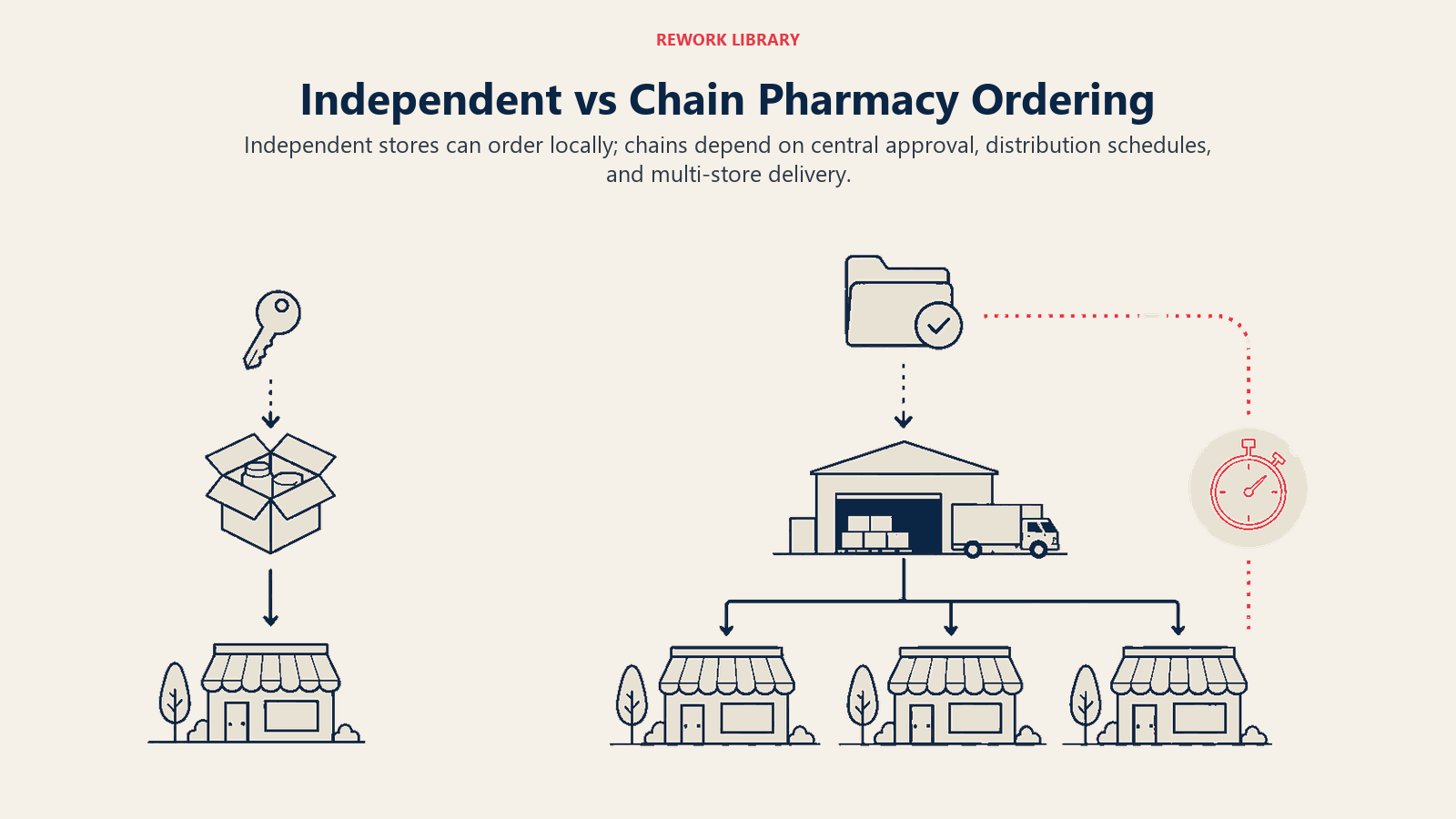
Independent Pharmacy: The pharmacist owner or manager typically controls purchasing decisions directly. They can place an order during your visit. The decision-maker is present, and the order can be placed in real time. The conversation about stock, reorder quantity, and distributor confirmation happens in one interaction.
The relationship dynamic in independent pharmacy is personal. The pharmacist knows their customer base, their sell-out patterns, and their cash flow constraints better than any system. The rep who understands the owner's economics (margin pressure, cash cycle, seasonal demand) can frame the order ask in terms that resonate at that level.
Chain Pharmacy: The pharmacist on duty rarely controls purchasing. Orders are generated by a central buying team using planogram data, category management systems, and store-level scan data. The in-store pharmacist may not be able to place a manual order even if they want to.
In chain environments, the rep's influence on inventory operates at two levels. At the outlet level, the rep can flag low-stock situations to the store manager or pharmacist for escalation to the buying team. At the corporate level, key account engagement with the central buying team determines auto-replenishment thresholds and promotional stock allocations.
Understand which model governs each pharmacy in your territory before every visit. Presenting a reorder ask to a chain pharmacist who has no purchasing authority wastes both parties' time and signals a lack of operational sophistication.
Stockout Recovery Protocol
A stockout discovered mid-visit requires a response, not a consolation. Here's the decision framework:

Step 1: Confirm the full extent. Check shelf, back room, and open orders. Is this a true zero-inventory situation, or are there units in transit?
Step 2: Estimate the patient impact window. How many days will the pharmacy be without stock? Does the delivery cycle fill the gap, or is the pharmacist actively turning away prescriptions?
Step 3: Activate emergency replenishment. Call your distributor immediately from the pharmacy. Most distributors have expedited delivery protocols for stockout situations. Confirm the order and estimated delivery date before leaving the outlet.
Step 4: Provide interim bridge options. If a neighboring pharmacy (independent or chain) in the immediate area carries your product, confirm availability. Some pharmacists will refer patients to a nearby outlet rather than substitute. This protects the script even if it doesn't count as your outlet's sale.
Step 5: Document and debrief. Log the stockout event in your CRM with date, product, estimated lost scripts, and recovery actions taken. Report to your field manager. Stockout patterns across multiple outlets may indicate a distributor coverage gap or a territory routing problem that management needs to address. A systematic review of medicine stockouts found that distribution barriers and weak supply chain information management were the most frequently cited root causes, exactly the patterns territory data can surface.
Step 6: Adjust future safety stock. Increase the safety stock threshold for this pharmacy and product combination. A stockout event is evidence that the previous threshold was insufficient for actual demand.
| Situation | Immediate Action | Within 24 Hours |
|---|---|---|
| Zero stock, no open order | Place emergency order via distributor | Confirm delivery date, notify pharmacist |
| Zero stock, order placed | Confirm ETA, offer bridge referral | Follow up on delivery completion |
| Zero stock, in transit | Give pharmacist ETA, flag expedite if needed | Verify stock arrival on next pass |
| Low stock, above safety threshold | Place reorder now, note pattern | None, unless sell-out accelerates |
CRM Logging for Stock Data
Stock data captured in the field has no commercial value unless it's logged consistently and accessible to management. The CRM visit record for every pharmacy call should include:
- Units on shelf by SKU (mandatory)
- Back-room units by SKU (when confirmed)
- Date of last order placed (from pharmacist or distributor records)
- Recommended order quantity from cover-day calculation
- Order placed during visit (yes/no, quantity)
- Stockout events (yes/no, product, estimated duration)
- Distributor delivery confirmation status
Managers reviewing territory coverage need this data to identify patterns: which pharmacies are chronically under-stocked, which reps are consistently placing orders versus only auditing, and which distributor routes are generating repeat stockout events. The same principles that govern CRM data hygiene in sales operations apply here: a field record is only useful if it is complete, consistent, and entered at the point of activity rather than reconstructed hours later.
Frequency expectation: stock data should be logged on every pharmacy visit, not just visits where an order was placed. An "all clear" log entry (stock above threshold, no order needed) is as valuable as an order confirmation because it establishes the baseline trajectory between events.
Field teams using structured stock management disciplines report higher coverage frequency at pharmacies with higher ordering rates, because pharmacists who associate rep visits with inventory problem-solving grant access more readily than pharmacists who view rep visits as interruptions.
Frequently Asked Questions about Pharmacy Order and Stock Management
What is a cover-day calculation and why does it matter for pharma reps?
A cover-day calculation tells a rep how many days of stock a pharmacy currently holds for a given product based on its actual sell-out rate. The formula is: Cover Days = (Units on Hand + Back-Room Units) / Daily Sell-Out Rate. It matters because it turns a vague "looks low" shelf observation into a precise, defensible reorder conversation. A rep who arrives with a specific cover-day number is making a business case; a rep who guesses is making a request.
How do I set safety stock thresholds for different pharmacy accounts?
Safety stock is account-specific and product-specific. The formula is: Safety Stock = Daily Sell-Out Rate x Lead Time Days x Buffer Factor, where buffer factor is typically 1.25 to 1.5 depending on how reliably your distributor delivers. Start by establishing the pharmacy's daily sell-out rate from secondary sales data or visit-to-visit stock observations. Then confirm the distribution lead time for that account's territory. High-traffic pharmacies and products with variable demand warrant buffer factors toward the upper end of that range.
What should I do when a pharmacist says the distributor will handle stock automatically?
This is the most common deflection, and it requires verification, not acceptance. The right follow-up question is: "Is there an open order on your account with the distributor for this product right now, or are you expecting them to read the shelf and replenish automatically?" Many distributors do not auto-replenish without an explicit order. If the pharmacist isn't certain, offer to call the distributor directly from the counter to confirm or place the order. This takes two minutes and removes ambiguity without creating friction.
How does the ordering process differ between independent and chain pharmacies?
In independent pharmacies, the owner or manager typically controls purchasing and can place an order during your visit. The conversation about stock, reorder quantity, and distributor confirmation happens in one interaction. In chain pharmacies, the pharmacist on duty rarely controls purchasing. Orders flow from a central buying team using planogram data and scan information. At the outlet level, you can flag low-stock situations for escalation; at the corporate level, a key account team negotiates auto-replenishment thresholds. Knowing which model governs each pharmacy before the visit avoids wasting either party's time.
How much stock data should I log after every pharmacy visit?
Every visit should capture: units on shelf by SKU, back-room units when confirmed, date of last order placed, recommended order quantity from the cover-day calculation, whether an order was placed during the visit (and how many units), any stockout events, and distributor delivery confirmation status. An "all clear" log entry is as valuable as an order confirmation because it establishes the baseline trajectory between visits. Managers reviewing territory coverage rely on this data to identify chronic under-stocking patterns and distributor coverage gaps.
What causes most pharmacy stockouts and how can reps prevent them?
Research published in PubMed (PMC9287964) identifies distribution barriers and weak supply chain information management as the most frequently cited root causes of stockouts. At the rep level, prevention comes down to three behaviors: consistent in-visit stock audits that catch low-stock trajectories before they reach zero; specific order asks with a calculated reorder quantity; and direct distributor confirmation rather than assuming scheduled delivery will include your product. Reps who own all three behaviors see materially fewer stockout events than those who treat stock as the distributor's problem.
The Cover-Day Reorder Model is the core stock management method described in this article: calculate daily sell-out rate from secondary sales data, divide total on-hand inventory by that rate to get cover days, compare cover days to the distribution cycle length, and trigger a specific order ask any time cover days fall below 1.5x the cycle length. The model converts a shelf observation into a defensible business case the pharmacist can act on immediately.
Pharmacies managed under the Cover-Day Reorder Model generate three compounding advantages. First, the rep arrives with a specific reorder quantity rather than a vague suggestion, which increases order conversion. Second, the pharmacist associates each rep visit with a useful operational outcome, not an interruption, which improves access over time. Third, consistent data logging surfaces stockout patterns that distributor reports alone would never catch, giving commercial managers the intelligence they need to address territory-level supply problems.
A second point worth noting: the buffer factor in the safety stock formula is not set once and forgotten. A pharmacy that experiences a stockout has just told you its previous buffer was too low. The correct response is to increase the safety stock threshold for that product-account combination before the next visit, not to note the incident and move on.
Conclusion: The Shelf Is the Scorecard
Stock on the shelf is the precondition for everything else in the field sales playbook. Detailing drives prescriptions. Prescription pull-through drives pharmacy recommendations. But recommendations require product. None of it works if the shelf is empty when the patient walks in.
The field rep who treats stock management as an operational chore, something to check off before getting to the "real" sales conversation, will consistently lose scripts to stockouts that a more disciplined competitor would have prevented.
The rep who owns inventory as a revenue protection activity, building the cover-day calculation into every visit, making the specific order ask, confirming with the distributor, and logging everything, gives every commercial investment made upstream (detailing, sampling, promotional spend) a fighting chance to convert into actual sales.
Stock is not logistics. Stock is revenue.
Learn More

Senior Implementation Consultant
On this page
- Who Actually Owns the Stock Problem in Pharmacy Sales?
- The In-Visit Stock Audit
- Shelf Count
- Back-Room Check
- Safety Stock Threshold
- Reorder Triggers and the Order Ask
- Cover-Day Calculation
- The Reorder Conversation
- Handling the "Distributor Will Deliver" Deflection
- Order Size Optimization
- Independent Pharmacy vs. Chain Pharmacy Ordering Dynamics
- Stockout Recovery Protocol
- CRM Logging for Stock Data
- Conclusion: The Shelf Is the Scorecard
- Learn More