Field Reporting and Closed-Loop Marketing: Turning Rep Activity into Actionable Commercial Intelligence
 There's a persistent intelligence gap in most pharma commercial operations. Your reps visit 8 to 12 health care professionals (HCPs) a day. They show slides, leave samples, discuss clinical data, and gauge reactions in real time. That's hundreds of HCP interactions per week across your field force, each containing signals about which messages resonate, which objections keep coming up, and which HCPs are shifting their prescribing intent.
But when marketing meets to plan the next campaign cycle, they're working from call volume reports and aggregate prescribing data. They don't know which slides lost the doctor's attention. They don't know that three regional managers are hearing the same pricing objection in every oncology call. They don't know that the patient support materials are generating more HCP questions than the clinical dossier.
There's a persistent intelligence gap in most pharma commercial operations. Your reps visit 8 to 12 health care professionals (HCPs) a day. They show slides, leave samples, discuss clinical data, and gauge reactions in real time. That's hundreds of HCP interactions per week across your field force, each containing signals about which messages resonate, which objections keep coming up, and which HCPs are shifting their prescribing intent.
But when marketing meets to plan the next campaign cycle, they're working from call volume reports and aggregate prescribing data. They don't know which slides lost the doctor's attention. They don't know that three regional managers are hearing the same pricing objection in every oncology call. They don't know that the patient support materials are generating more HCP questions than the clinical dossier.
Turn this article into takeaways for your work.
Each assistant summarizes the article only for you and suggests best practices for your work.
Closed-loop marketing (CLM) exists to close that gap. Field reporting is the mechanism that makes it work.
What Closed-Loop Marketing Actually Means in Pharma
Key Facts: Closed-Loop Marketing
- A Deloitte analysis found that while 80% of pharma executives rated their customer engagement strategies positively, only 35% of HCPs agreed that pharma's customer-facing resources met their needs, a gap that interaction-driven CLM programs directly address (Deloitte, 2024)
- Call reports submitted at the end of the day capture what reps remember through nine hours of subsequent interactions; real-time reporting within 30 minutes of each visit consistently produces higher data accuracy and completeness, a pattern pharma CRM teams widely observe in same-day versus batch-reporting comparisons
- The OIG Compliance Program Guidance for pharmaceutical manufacturers identifies clear organizational accountability, including ownership of the feedback loop from field data to brand decisions, as a foundational element of any compliant commercial operation
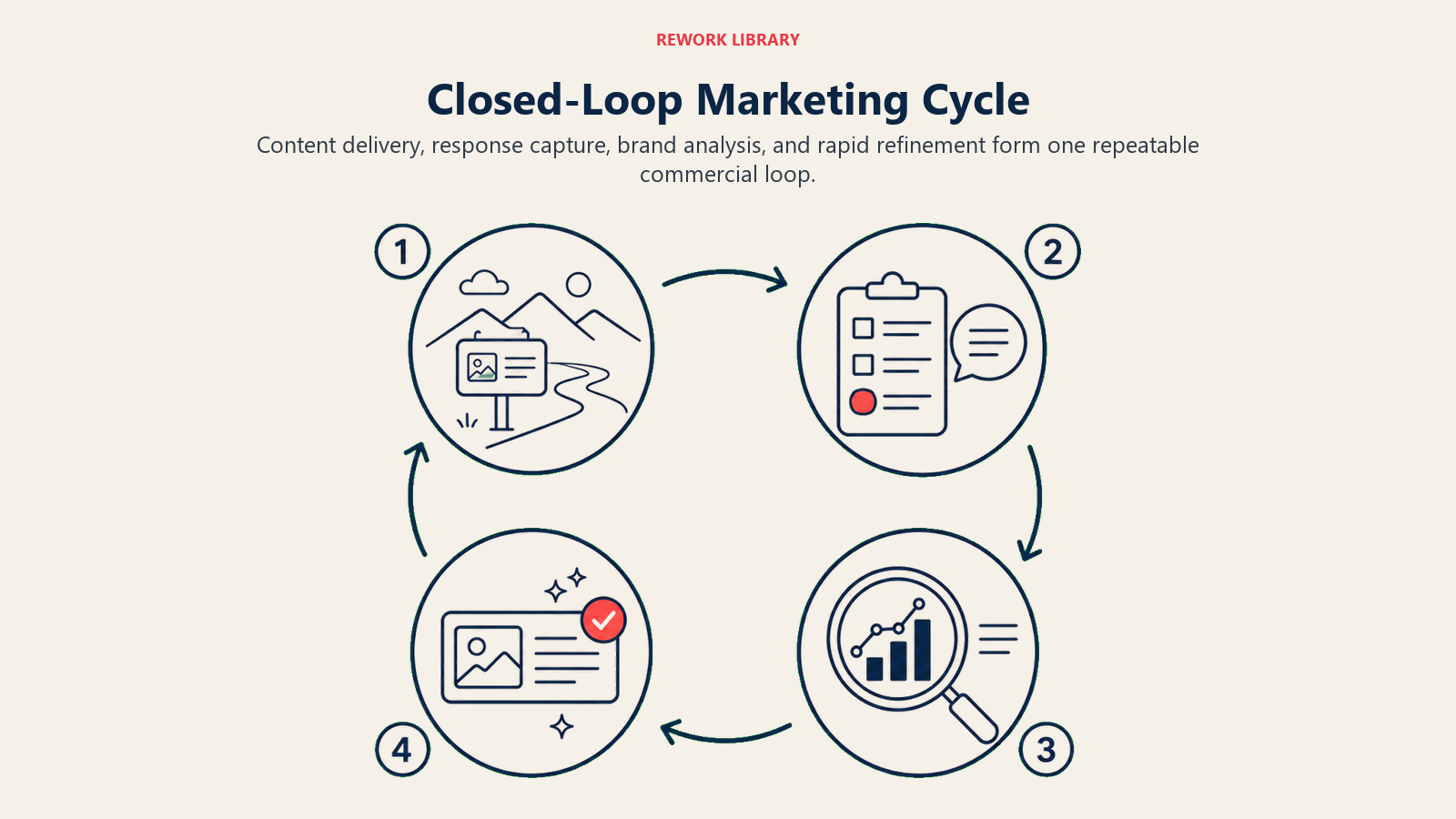
CLM in pharma is a systematic cycle with four steps: deliver content to HCPs through field interactions, capture HCP response data at the point of delivery, analyze that response at the brand level, and refine targeting and messaging based on what the data reveals. Then deliver again, with the next version of content optimized by what you learned.
The "loop" is between the field and the brand team. Without a mechanism to close it, every detailing cycle starts fresh, and the field learns things the brand never knows.
Traditional detailing was static: reps carried printed visual aids, delivered a scripted message, and reported back on what the HCP said. The information transfer was one-way, the content couldn't adapt mid-cycle, and the feedback mechanism was the rep's memory filtered through a call report written hours later.
CLM through tablet-based e-detailing platforms changes this in three ways. First, content is digital and can be updated between cycles without reprinting. Second, the platform captures interaction data automatically: which slides were shown, how long each slide was on screen, whether the HCP engaged with embedded questions, and which materials were requested at close. Third, that interaction data syncs to the CRM and analytics layer, where it becomes structured commercial intelligence instead of anecdote.
The rep's role doesn't shrink. If anything, it expands. The rep brings clinical expertise and relationship knowledge that no platform can replicate. But the platform captures what happens during the conversation in ways a rep can't self-report accurately.
Field Reporting Fundamentals
The Closed Detailing Loop is the four-stage CLM cycle in pharma: deliver digital content through field interactions, capture HCP response data automatically at the point of delivery, aggregate and analyze that response at the brand level, and refine targeting and content before the next call cycle. The loop is only as fast as its slowest stage. Organizations with 12-week MLR content review cycles deliver content updates that are already three or more call cycles behind the market conversation that prompted them (where a typical call cycle runs 4 to 6 weeks). A call report is the basic unit of field intelligence. Done well, it takes a rep 60 seconds to complete and gives sales ops and brand teams a precise record of every HCP interaction. Done poorly, it's a compliance checkbox that captures nothing useful.
The Structure of a Good Call Report
A well-designed call report captures six things:
- HCP visited: pre-populated from CRM, confirmed by rep
- Products discussed: checklist selection, not free text
- Materials shown: auto-populated from CLM platform (slides shown, time spent per slide)
- Samples distributed: quantities by product, tied to e-signature capture
- HCP reaction: brief structured field (interested, neutral, objection, requested follow-up) plus optional free-text notes for anything unusual
- Next steps: agreed action for next visit, set as a scheduled task in CRM
Six fields. Most of them pre-populated or checkbox-based. The CLM platform handles the materials and engagement data automatically. The rep confirms and submits.
Compare that to call reports with 15 to 20 free-text fields, and you understand why rep compliance with reporting requirements often sits at 60 to 70% rather than 95% or better. Every field you add that requires rep effort is a field you'll get inconsistent data in.
Compliance Requirements in Call Reporting
Sample documentation and fair balance compliance aren't optional, and they create specific reporting requirements that CLM and SFA systems must handle correctly.
Sample transactions require: the HCP's DEA or license number (verified against the HCP record), the quantity and lot number of samples distributed, and a valid e-signature captured at point of delivery. Reports submitted without completed sample documentation are audit exposure under the FDA Prescription Drug Marketing Act, which sets federal requirements for sample record-keeping and prohibits unauthorized distribution. Systems that allow reps to submit call reports without completing sample fields create systematic compliance gaps.
Fair balance compliance means that when a rep discusses product benefits, the call report and the CLM platform need to reflect that risk and side effect information was also presented. Some platforms are configured to encourage or require that fair balance slides be shown before or alongside clinical benefit slides, though how strictly this is enforced is typically a brand-level content architecture decision rather than a universal platform default. Others flag call reports for manager review when benefit slides are shown without corresponding risk disclosure records. Both approaches work. What doesn't work is relying on reps to self-report fair balance compliance accurately under time pressure.
Real-Time vs. Batch Reporting
A call report submitted 30 minutes after a visit captures what actually happened. A call report submitted at 9pm for calls made between 8am and 5pm captures what the rep remembers, filtered through nine hours of subsequent interactions and road time.
Real-time reporting, supported by an offline-capable mobile app, is the standard that produces reliable field intelligence. Batch reporting at day's end is the standard that produces attendance records dressed up as call reports.
The argument against real-time reporting is usually rep time: if they're submitting a call report in the parking lot after every visit, they're not maximizing face time with HCPs. This is true if the call report takes 5 minutes. It's not true if it takes 60 seconds, which is achievable when the platform is designed correctly.
Manager coaching quality also depends on reporting timeliness. A first-line manager reviewing a rep's day in the afternoon can provide same-day coaching on a difficult objection or an HCP who showed unusually high interest. A manager reviewing yesterday's batch upload can't.
Closed-Loop Marketing in Practice
Content Performance Tracking
The most immediate value CLM platforms provide is content performance data: which slides reps showed most, which they skipped, how long HCPs spent engaging with each module, and which content drove the most requests for follow-up materials or clinical references. This data reveals things that aggregate call volume numbers never will. You might find that:
- The competitive differentiation module is consistently skipped in primary care calls but shown in nearly every specialist call
- The disease burden slide holds HCP attention for an average of 2.3 minutes, while the clinical trial efficacy slide averages 47 seconds
- Reps in Region 3 are showing the patient support materials in 85% of calls while reps in Region 5 show them in 12% of calls
- The new pricing module that launched in Q2 is generating HCP questions in 40% of calls, suggesting either an opportunity or a communication gap
None of this is visible without content engagement tracking. And none of it can be acted on without connecting content data back to the brand team.
HCP Segmentation Updates Triggered by Interaction Data
Traditional HCP segmentation is static: you assign each HCP to a tier based on prescribing volume and specialty, and that assignment stays until the next quarterly review. CLM data makes segmentation dynamic.
When an HCP who's classified as a low-potential B-segment doctor spends 4 minutes engaging with clinical data, requests a patient support kit, and asks for a medical science liaison visit, the system should flag that HCP for potential tier upgrade without waiting for a quarterly review cycle. A Deloitte analysis of pharma HCP engagement found that while 80% of pharma executives rated their customer engagement strategies positively, only 35% of HCPs agreed that pharma's customer-facing resources met their needs, a gap that interaction-driven segmentation directly addresses. When an A-segment HCP starts declining visits and disengaging from content, the system should flag that pattern for manager attention before prescribing data reflects the shift. The behavioral signals that drive these reclassifications work similarly to lead scoring systems in B2B sales: a weighted combination of recency, engagement depth, and intent indicators tells you who deserves more attention right now, without waiting for a calendar-driven review.
Interaction-triggered segmentation updates mean your reps are calling on the right HCPs based on current engagement signals, not on last quarter's prescribing data.
Feedback Loops from Field to Brand Teams
The most underused element of CLM programs is the feedback mechanism from field to brand. Most organizations use CLM data to measure what happened; fewer use it to systematically change what happens next.
A functional feedback loop works like this: CLM data is aggregated weekly and reviewed by brand teams in a structured format. The review covers content engagement rates (which slides perform), objection patterns (what HCPs are pushing back on), and regional variation (where messaging is landing differently). Based on that review, the brand team makes content updates, adjusts messaging emphasis, or flags recurring objections for medical and market access teams to address. Updated content is pushed to rep devices before the next call cycle begins.
The cycle time matters. A feedback loop with a 12-week lag produces content updates that are three or more call cycles behind the current market conversation (given typical 4 to 6-week call cycles). A feedback loop with a 2-week lag produces content that reflects what's actually happening in the field. This kind of structured review rhythm is a recurring, owned process that turns raw field signals into decisions, with accountability for who acts on what and by when.
Connecting Field Data to Marketing Decisions
How CLM Data Informs Next Best Action
Next best action (NBA) recommendations are the operational output of a well-functioning CLM system. Based on an HCP's interaction history, prescribing trend, current segmentation, and recent call outcomes, the system recommends what a rep should focus on in the next visit: which product to detail, which content module to open with, whether to leave samples or ask for a commitment.
NBA recommendations work when they're based on actual HCP behavior data, not just segment averages. An HCP who consistently engages with patient case study content should get a different recommended approach than an HCP who engages primarily with clinical data, even if they're in the same prescribing tier.

Linking HCP Digital Touchpoints with Rep Visit Data
Many HCPs now engage with pharma brand content through channels outside of rep visits: email, branded portals, webinars, and medical education platforms. When a rep visits an HCP on Tuesday and that HCP opens a brand email and downloads a clinical reference on Thursday, those are two data points in the same HCP engagement story.
Omnichannel commercial operations link those touchpoints. An HCP who opens every email but has been declining rep visits for two cycles is a different situation than an HCP who's ignoring digital content and accepting every visit. The combined view lets commercial teams allocate resources and content by actual engagement pattern rather than channel-by-channel assumption.
This integration requires a common HCP identifier across channels, which most organizations manage through a master data management layer. The work is technical and often underestimated, but it's what separates omnichannel from multi-channel.
Coordination Between Field and Non-Personal Promotion
Non-personal promotion (NPP) includes digital advertising, email campaigns, peer-to-peer programs, and medical education events. It reaches HCPs between rep visits and can prime or reinforce field detailing messages.
Coordinating NPP with field activity means: reps know which HCPs are actively engaged with digital campaigns before they visit, digital campaigns can be triggered or suppressed based on recent rep call records, and the timing of NPP touchpoints can be aligned with field call cycles so HCPs aren't receiving conflicting messages from the same brand through different channels in the same week.
The connection between CLM and NPP coordination is the topic we expand on in Doctor Detailing Best Practices and the use of Detail Aid and Visual Aid Usage as part of a coherent HCP communication strategy.
Common CLM Pitfalls
Rigid content locked by medical and regulatory review cycles. The CLM promise is adaptive content. The reality in many organizations is content that goes through 12-week review cycles and can't be updated between them. When the market moves faster than your MLR process, your CLM system becomes a sophisticated way to deliver the same static message your printed aids would have delivered. The fix isn't bypassing medical review. It's modularizing content so that low-risk updates (pulling a slide, updating a statistic, reordering a module) don't require the same review cycle as new clinical claims.
Poor analytics adoption by brand teams. CLM platforms generate data. Generating data and using data are different things. Many CLM implementations produce weekly reports that get glanced at and filed. The organizations that extract value from CLM make content performance review a standing agenda item in brand team meetings, with a designated person responsible for translating data into recommended actions.
Data silos between CLM and CRM. If call records live in one system and content engagement data lives in another with no automatic sync, someone has to manually join those datasets to answer any meaningful commercial question. Manual data joins happen irregularly, with lag, and usually only when a director asks a question that can't be answered without them. Integration between CLM and CRM should be real-time and bidirectional.
Governance: Who Owns the CLM Process
CLM sits at the intersection of sales operations, brand marketing, medical, regulatory, and IT. That intersection is where ownership fights happen, which is why most CLM governance failures are organizational, not technical. A governance model that works assigns clear ownership at each stage of the CLM cycle. The OIG Compliance Program Guidance for pharmaceutical manufacturers identifies clear organizational accountability as a foundational element of any compliant commercial operation, which maps directly onto the CLM ownership structure:
| Stage | Owner | Supporting Roles |
|---|---|---|
| Content creation and update | Brand marketing | Medical, regulatory, market access |
| MLR review and approval | Medical, regulatory | Brand marketing |
| Platform configuration and content loading | Commercial ops / IT | Sales ops |
| Field deployment and training | Sales ops | First-line managers |
| Usage monitoring and rep compliance | Sales ops | First-line managers |
| Data analysis and reporting | Commercial analytics | Brand marketing |
| Insight-to-action decisions | Brand team | Commercial ops, field leadership |
The gap most organizations leave is the "insight-to-action" step. Data gets analyzed. Insights get presented. And then nothing changes until the next campaign cycle. Governance should specify who is accountable for translating CLM insights into content updates or messaging adjustments, and on what timeline. For broader alignment between field and brand, see Marketing and Field Sales Alignment.
KPIs for CLM Programs
| KPI | What It Measures | Why It Matters |
|---|---|---|
| Content engagement rate | % of HCPs who engage with each module during a call | Identifies which content resonates vs. which gets skipped |
| Message pull-through rate | % of calls where key brand message was delivered and confirmed | Measures whether reps are using CLM as designed |
| HCP segment shift rate | % of HCPs who moved to a higher segment after CLM interaction | Connects engagement data to segmentation decisions |
| CLM-to-call correlation | % of calls where CLM platform was used vs. unrecorded verbal detail | Measures CLM adoption vs. traditional detailing fallback |
| Feedback loop cycle time | Days from field data capture to content update deployment | Measures how fast the loop actually closes |
| Post-visit digital engagement | % of visited HCPs who engage with NPP within 14 days | Measures omnichannel coordination effectiveness |
The connection between these KPIs and broader Pharma CRM and Sales Force Automation metrics is important: CLM KPIs answer "what content is working," while CRM KPIs answer "where is the field investing time." Together they answer "is the right time being invested in the right HCPs with the right content."
And ultimately, both feed into territory analytics dashboards that give commercial leadership the full picture of field force effectiveness.
The organizations that close this loop reliably aren't always the ones with the most sophisticated platforms. They're the ones that made "insight to action" a standing agenda item with a named owner and a defined timeline, not an aspirational outcome at the end of a CLM implementation deck.
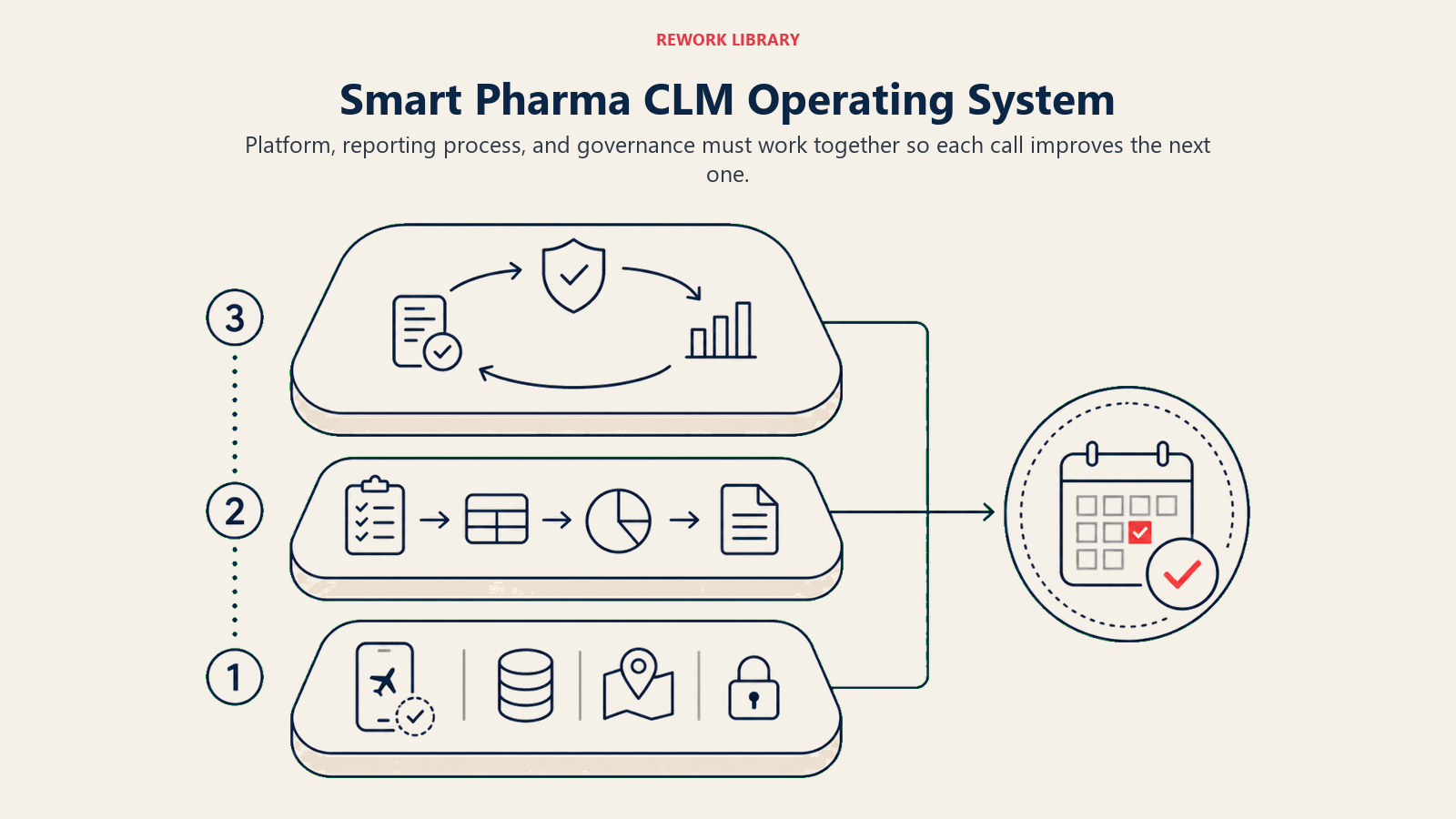
A Field Reporting and CLM System That Makes Every Rep Visit Smarter
The ambition of closed-loop marketing is straightforward: each rep visit should be informed by what happened in the last one, and each brand content decision should be informed by what's happening in the field right now. Getting there requires investment in three layers: the platform (offline-capable CLM with CRM integration), the process (call report design that captures signal without burdening reps), and the governance (ownership of the feedback loop from field data to brand decisions). Organizations that build all three layers turn their field force into a commercial intelligence operation that gets smarter with every call cycle. Organizations that build the platform without the process and governance get expensive reporting software that generates data nobody acts on.
The rep who walks into an HCP office with an NBA recommendation based on that HCP's last three interactions, their recent digital engagement, and the current competitive landscape in their prescribing segment is a more effective rep than one walking in with a standard slide deck and a sales target. CLM is what makes that rep possible.
Frequently Asked Questions about Field Reporting and Closed-Loop Marketing
What is closed-loop marketing in pharma and how is it different from traditional detailing?
Traditional detailing was static: reps carried printed materials, delivered a scripted message, and reported back verbally or in a text note hours later. CLM adds three things: digital content delivered on a tablet that adapts between cycles, automatic capture of HCP interaction data (which slides were shown, how long each was on screen, what was requested), and a structured feedback mechanism that routes that data back to brand teams for content and targeting updates. The loop is closed when the brand acts on field data before the next detailing cycle begins.
How should a call report be designed to maximize data quality?
Six fields, most pre-populated. HCP identity and last visit data come from the CRM. Materials shown and time-per-slide come from the CLM platform. Sample quantities and e-signature flow from the SFA module. The rep confirms, adds a brief HCP reaction field (interested, neutral, objection, or requested follow-up), sets a next step, and submits. Anything above 10 manual fields drives rep abandonment and inconsistent data. The call report should take 60 seconds to complete, not five minutes.
What compliance documentation does a call report need to capture?
For sample transactions: the HCP's DEA or license number verified against the HCP master record, the quantity and lot number of each sample type distributed, and a valid e-signature captured at point of delivery. For clinical content: evidence that fair balance information (risk and side effects) was presented alongside product benefit content. Systems that allow reps to submit without completing sample documentation create systematic audit exposure under the FDA Prescription Drug Marketing Act. For fair balance, some organizations configure CLM platforms to flag or prompt fair balance presentation alongside clinical benefit content, though the specific enforcement approach is typically a brand-level decision.
How quickly should CLM feedback reach brand teams?
A two-week cycle is achievable and commercial. A 12-week cycle is not. Modularizing content so that low-risk updates such as pulling a slide, updating a statistic, or reordering a module do not require a full MLR review is the key to faster loops. New clinical claims need full review. A slide sequence change or a supporting statistic update generally does not. Organizations that treat every content edit as a full regulatory submission produce CLM systems that adapt no faster than their printed visual aids did.
What is the difference between CLM and omnichannel marketing?
CLM covers the loop between rep field visits and brand content decisions. Omnichannel marketing adds non-personal promotion channels (email, branded portals, medical education platforms, peer-to-peer programs) and links their engagement data to the same HCP record as rep call data. An HCP who opens every brand email but has been declining rep visits for two cycles is a different engagement situation than one who accepts every visit but ignores digital outreach. Omnichannel gives commercial teams both data points; CLM alone gives them only the in-person view.
Who should own the CLM feedback loop in a pharma commercial organization?
Ownership of the insight-to-action stage, where CLM data is translated into content updates or targeting adjustments, should sit with the brand team with a designated individual accountable for review and decision timelines. Usage monitoring and rep compliance belong to sales operations. Platform configuration and content loading belong to commercial operations or IT. Medical and regulatory own MLR review. The most common governance failure is leaving the insight-to-action step unassigned: data gets analyzed, insights get presented, and nothing changes until the next campaign cycle.
Learn More

Senior Implementation Consultant
On this page
- What Closed-Loop Marketing Actually Means in Pharma
- Field Reporting Fundamentals
- The Structure of a Good Call Report
- Compliance Requirements in Call Reporting
- Real-Time vs. Batch Reporting
- Closed-Loop Marketing in Practice
- Content Performance Tracking
- HCP Segmentation Updates Triggered by Interaction Data
- Feedback Loops from Field to Brand Teams
- Connecting Field Data to Marketing Decisions
- How CLM Data Informs Next Best Action
- Linking HCP Digital Touchpoints with Rep Visit Data
- Coordination Between Field and Non-Personal Promotion
- Common CLM Pitfalls
- Governance: Who Owns the CLM Process
- KPIs for CLM Programs
- A Field Reporting and CLM System That Makes Every Rep Visit Smarter
- Learn More