Distributor and Stockist Management: Keeping the Pharma Supply Chain Moving
Turn this article into takeaways for your work.
Each assistant summarizes the article only for you and suggests best practices for your work.
A medical rep spends two hours with a cardiologist. The conversation goes well: the doctor is convinced, she prescribes, the patient arrives at the pharmacy the next morning. And the product isn't on the shelf.
That scenario plays out across pharma markets every day. The field force did everything right. The detailing was strong. The prescription was written. But distribution broke the chain, and the patient either waits, switches brands, or walks away. Every stock-out is a prescription that didn't convert into a sale. And every prescription that didn't convert is detailing investment that generated zero return.
Distribution management isn't a logistics function sitting downstream of commercial. It's the mechanism that determines whether commercial activity translates into revenue. Pharma companies that treat distributors and stockists as passive logistics providers leave money on the table and, more importantly, leave patients without the products their doctors recommended.
Distributor vs Stockist vs Wholesaler: Getting the Definitions Right
These three terms get used interchangeably in markets where they mean very different things. Getting them straight matters because each channel partner has different coverage expectations, margin structures, and management requirements.
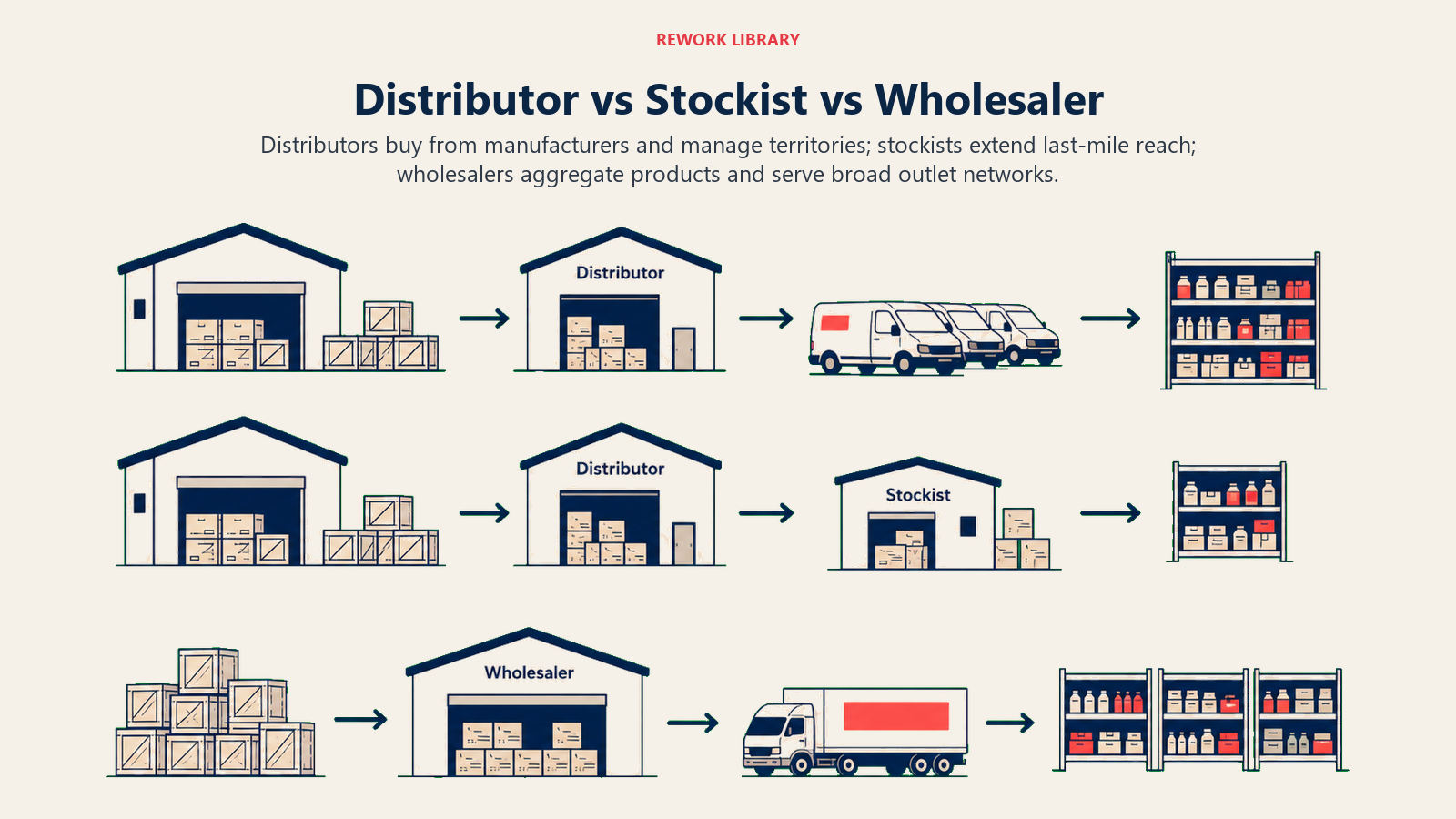
Distributors hold primary stock, typically purchased directly from the manufacturer or national importer. They cover defined geographic territories, manage their own van sales teams, and are responsible for secondary distribution to pharmacies, drug stores, clinics, and hospitals within their territory. A distributor usually carries credit risk on downstream customers. They're your frontline commercial partners: they warehouse, they sell, and they collect.
Stockists (also called sub-distributors or C&F agents in some markets) sit one level below distributors in many channel configurations. They hold stock transferred from a primary distributor and service a narrower catchment, often a single city or district. A stockist's margin is typically thinner than a distributor's because they bear less risk and cover less geography, but they provide last-mile reach into areas a distributor's van sales team can't efficiently service.
Wholesalers operate differently. They aggregate product from multiple manufacturers, carry broader but shallower portfolios, and typically don't do active selling. Pharmacies buy from them for convenience, not brand preference. Wholesalers matter for generic products and over-the-counter lines, but for prescription brands where detailing drives demand, relying on wholesale as a primary channel is a mistake.
| Channel Type | Coverage Scope | Illustrative Margin Range | Active Selling | Stock Ownership |
|---|---|---|---|---|
| Primary Distributor | Territory (multi-district) | 8-15% (varies widely by market and category) | Yes (van sales) | Owned |
| Stockist / Sub-distributor | City / district | 4-8% (market-dependent) | Limited | Owned |
| Wholesaler | Multi-manufacturer | 2-5% (market-dependent) | No | Owned |
| C&F Agent | State / region | 2-4% (market-dependent) | No | Held on behalf |
Margin ranges above are illustrative of typical structures in South and Southeast Asian pharma markets; actual figures vary significantly by country, product category, negotiating leverage, and credit risk allocation. The right channel configuration depends on your geographic ambitions and portfolio mix. A prescription-focused specialty portfolio typically runs through primary distributors with selective stockist depth in high-potential cities. An OTC-heavy portfolio needs broader reach, which often means layering in wholesaler coverage.
Key Facts: Distributor and Stockist Management
- Research on drug shortages shows drug use reductions during shortage events ranging from 1% to 99%, making the commercial and patient-safety stakes of distribution failures concrete (PMC12215599).
- WHO good distribution guidelines specify that every party in the distribution chain must maintain temperature control and environmental monitoring throughout storage and transport, a compliance obligation that sits with the distributor, not just the manufacturer (WHO Good Distribution Practices).
- Research on drug shortages in the US Veterans Health Administration found facilities turning to gray-market channels during supply gaps, with documented markups of 300% to 500% above baseline pricing, illustrating the cost consequences when authorized supply chains fail (PMC6248141).
Distributor Selection Criteria: What Actually Matters
Selecting a distributor is one of the highest-leverage decisions a pharma commercial leader makes. The wrong distributor costs you months of market access and, once appointed, is politically difficult to replace. The right one becomes a genuine commercial extension of your field force. The Distributor Fitness Framework structures this decision across six dimensions: geographic coverage (actual versus claimed), financial health, van sales team capability, cold-chain infrastructure, portfolio conflict exposure, and reputation with pharmacies. Weighting these dimensions before evaluating candidates prevents the most common selection mistake, which is choosing on coverage claims and margin appetite without validating operational capability.
Geographic reach and outlet coverage: Does the distributor actually service the pharmacies, clinics, and hospitals in your target areas? Ask for a route list with outlet counts. Verify a sample. Distributors routinely overstate coverage, particularly in rural areas.
Financial health: A distributor who can't fund adequate stock levels will stock out during demand peaks. Ask for audited financials or at minimum a bank credit reference. Look for working capital relative to the stock value you expect them to hold. A distributor with thin margins, heavy borrowing, and a large multi-manufacturer portfolio is a stockout risk.
Cold-chain capability: For biologics, vaccines, and temperature-sensitive formulations, cold-chain competence is non-negotiable. Inspect the facility. Check the temperature logging system. Ask how they handle a power failure during storage. Don't take claims at face value. WHO distribution guidelines specify that every party in the distribution chain must maintain temperature control and environmental monitoring throughout storage and transport.
Existing portfolio conflicts: A distributor who already holds a competing brand in your therapeutic category has an inherent incentive conflict. They may still be a good partner, but you need to negotiate explicit shelf space and push activity commitments up front, or find a distributor without the conflict.
Van sales team quality: Distributors don't just warehouse product. In most pharma markets, their van salespeople (often called "salesmen" or "field reps") are the ones taking orders from pharmacy counters. How many do they have? What's their call frequency? Do they have handheld order management devices? A distributor's van sales capability is a direct multiplier of your market penetration.
Scorecard: Distributor Selection
| Criterion | Weight | What to Evaluate |
|---|---|---|
| Geographic coverage (actual vs claimed) | 25% | Route list audit, outlet sample check |
| Financial health | 20% | Working capital, payment history with current suppliers |
| Van sales team size and frequency | 20% | Headcount, average calls per day, order capture method |
| Cold-chain infrastructure | 15% | Facility inspection, temperature monitoring system |
| Portfolio conflict exposure | 10% | Competing brands carried, willingness to commit share of voice |
| Reputation with pharmacies | 10% | References from pharmacy owners in territory |
Onboarding and Contracting: Setting the Relationship Up Right
A signed distribution agreement is where most pharma companies stop. Good ones use the contracting process to build the operational foundation of a commercial partnership.

Stock level commitments: The agreement should specify minimum stock cover at the distributor's warehouse, typically expressed as days of stock on hand based on your planned monthly offtake. A commonly recommended floor is 21 days of cover, with a ceiling of 45-60 days to limit expiry risk, these are contractual targets you negotiate, not published industry benchmarks. Calibrate against your product's demand volatility and distributor logistics capability. Below the floor, the distributor is expected to reorder. Above the ceiling, you or the distributor should investigate to prevent expiry risk.
Ordering and delivery SLAs: Specify order-to-delivery timelines for standard orders versus emergency replenishments. For temperature-sensitive products, require cold-chain documentation with every delivery. Build in a claims process for damaged or short-delivered stock.
Payment terms and credit exposure: Extended credit terms are often necessary to win a good distributor's business, but they create credit risk you need to manage. Specify the credit limit, payment terms, and the consequences of overdue accounts (typically supply hold after a defined grace period). The credit and margin negotiation that anchors a distributor agreement draws on the same fundamentals as any major commercial negotiation: the Negotiation Fundamentals framework is useful preparation for the commercial director entering multi-SKU, multi-territory distributor contracting discussions.
Secondary-sales reporting: This is where many pharma companies fail. You need secondary-sales data (what the distributor sells out to pharmacies and other customers) to track actual market penetration, not just your primary sales to distributors. Build the reporting requirement into the contract, define the format and frequency, and specify a data-sharing tool or template.
Stock rotation and expiry policy: Agree in writing who bears the cost of near-expiry product. A common structure is that the manufacturer accepts returns of product returned within 60 days of expiry, provided it was stored correctly and the return is supported by documentation. Distributor-held stock that expires without a return window specified will create disputes and trust erosion. The WHO good storage and distribution practices technical guidance covers stock rotation, repackaging controls, and documentation requirements that should anchor these contractual commitments.
SLA Clause Checklist for Distributor Agreements
- Minimum stock cover (floor and ceiling in days of stock on hand)
- Order-to-delivery lead time for standard and emergency replenishment
- Secondary-sales reporting format, frequency, and submission deadline
- Credit limit, payment terms, and overdue-account procedure
- Cold-chain documentation requirements for temperature-sensitive SKUs
- Near-expiry return window and condition for credit
- Territory exclusivity scope (if applicable) and conditions for review
- Key performance indicators that trigger a performance review
- Notice period and exit provisions
Performance Scorecard: Measuring What Matters
You can't manage a distributor relationship from gut feel. Build a monthly scorecard and review it in a structured business review. The metrics should be simple enough to collect consistently and specific enough to drive action.

Fill rate: What percentage of the orders your distributor receives from pharmacies and other customers are fulfilled in full? A fill rate below 90% is a common internal trigger for a performance conversation, indicating either inadequate stock levels or operational problems with order processing.
Order-to-delivery time: How long does it take from a pharmacy order to product on the shelf? Track this as an average and flag outliers. Long delivery times push pharmacies toward competing suppliers.
Stock-out frequency: How many times per month does the distributor report zero stock on a SKU? Stock-outs are the clearest signal that stock cover, ordering discipline, or your supply planning is broken. See Pharma Supply Chain and Inventory Visibility for a framework to diagnose stock-outs systematically.
Secondary-sales reporting compliance: Did the distributor submit their secondary-sales data on time, in the agreed format, and covering the agreed coverage period? Compliance below 100% is a data quality problem that undermines your ability to track market performance.
Expiry risk percentage: What share of the distributor's current stock is within 90 days of expiry? High expiry risk typically signals over-stocking of slow-moving SKUs or poor stock rotation.
| KPI | Target | Review Trigger |
|---|---|---|
| Fill rate (orders fulfilled in full) | >95% | Below 90% for two consecutive months |
| Order-to-delivery lead time | Under 48 hours (urban); under 72 hours (rural) | Any month exceeding target |
| Stock-out frequency per SKU | Zero per month | Any occurrence for primary SKUs |
| Secondary-sales reporting compliance | 100% on time | Any missed submission |
| Expiry risk percentage (current stock) | Below 5% by value | Any month above 8% |
Review this scorecard monthly with your distributor's senior contact, not just their order desk. Track trends. Distributors who consistently miss targets need a formal performance improvement conversation, not just a tighter SLA on the next order. Once the scorecard is working, the next question is how to structure the incentives that direct their commercial energy toward your priorities rather than the brand next to yours in their portfolio. See also Process KPIs for a clean structure for deciding which metrics are diagnostic versus outcome measures.
Incentive and Trade Terms Design
Margin alone doesn't motivate a distributor to push your brand versus the competing products in their portfolio. Well-designed incentives direct their commercial energy toward your priorities.
Volume rebates: Tiered rebates paid quarterly on primary-sales volumes are the most common incentive structure. A three-tier structure works well: a baseline rebate for reaching 80% of the quarterly target, a standard rebate for 100%, and an overachievement bonus for exceeding 110%. Keep the tiers achievable but requiring genuine effort.
Reach bonuses: Pay a separate bonus for active coverage of a defined outlet universe. If you want your distributor's van sales team visiting 500 pharmacies in their territory, set a quarterly reach bonus payable when they can demonstrate (via call data) that 90% of those outlets were visited and received an order in the quarter.
Co-investment in van sales: In high-potential territories, some manufacturers co-invest in dedicated van sales headcount aligned exclusively to their portfolio. This is expensive but creates a salesforce operating under your commercial priorities, not the distributor's portfolio mix priorities.
Target cascading to secondary sales: Link incentive payments to secondary-sales performance, not just primary offtake. A distributor who stockpiles product to hit primary-sales targets but can't move it to pharmacies isn't adding commercial value; they're creating future expiry risk. If your incentive scheme only rewards primary sales, you're incentivizing exactly this behavior.
Conflict and Escalation Management
Distributor relationships generate friction. Parallel imports, price undercutting, territory poaching, and product diversions are common problems that erode both margin and market structure. Having a defined escalation process prevents small problems from becoming relationship-ending disputes.
Parallel imports: Product moving from a lower-price market into a higher-price market through unauthorized channels undercuts your authorized distributors' margin and weakens their motivation to invest in your brands. Detect parallel imports through pack serialization, batch tracking, and monitoring of unusual price movements in the market. Address them through contract enforcement and, where necessary, supply restriction to the source market. Drug shortages caused by supply chain failures create conditions where unauthorized channels enter the market. Research on shortage impacts in the US Veterans Health Administration found facilities sourcing unavailable products through gray-market channels at documented markups of 300% to 500% above baseline pricing (PMC6248141). While that study focused on a US institutional setting, the dynamic, supply gaps opening the door to unauthorized and high-cost sourcing, applies across markets.
Price undercutting: When distributors undercut each other on price to win pharmacy business, it erodes trade confidence in your pricing structure. Build minimum pharmacy price commitments into distributor agreements and monitor through regular retail price audits. Some pharma companies use mystery shoppers or van sales app data to flag unusual discounting.
Territory overlap: Overlapping distributor territories create conflict over pharmacy accounts and tend to drive price competition. Define territories precisely in contracts, including the specific pharmacies assigned to each distributor where relevant, and specify what happens when a pharmacy on the border between two territories chooses to order from the non-assigned distributor.
The escalation path should go from your district sales manager (first response, within 24 hours) to your national distribution manager (formal review, within five business days) to a contract arbitration process if the first two levels don't resolve the issue. Document every step. The relationship work that prevents most escalations from reaching this point is where the real investment goes.
Distributor Relationships as a Strategic Asset
The best pharma commercial organizations don't manage distributors at arm's length. They treat top-tier distributors as co-investors in market development.
That means sharing demand data (prescription trends, doctor targeting lists, planned detailing activity) so distributors can anticipate demand rather than react to it. It means involving distributors in new product launch planning, not just notifying them of a launch date. And it means recognizing that a distributor's van sales team is, in most markets, the most frequent commercial contact a pharmacy owner has with your company.
A distributor who understands your strategy, trusts your data, and believes your incentive scheme is fair will push your brands when they're making the pharmacy-level selling decision. One who feels managed at arm's length with unrealistic targets and slow claims resolution will route their commercial energy toward brands and principals who treat them like partners.
The field force generates demand. Independent vs Chain Pharmacy Strategy determines how you capture it at the outlet level. But the distributor is the bridge between both. That bridge either holds or it doesn't, and whether it holds depends almost entirely on how you manage the relationship.
Frequently Asked Questions about Distributor and Stockist Management
What is the difference between a distributor and a stockist in pharma?
A distributor holds primary stock purchased directly from the manufacturer, covers a defined geographic territory, and manages its own van sales team to service pharmacies, clinics, and hospitals. A stockist (or sub-distributor) holds stock transferred from a primary distributor and services a narrower catchment, often a single city or district. Stockists provide last-mile reach where a distributor's van routes can't efficiently go, but they carry less credit risk and earn thinner margins.
What should a pharma company verify before appointing a distributor?
Six criteria matter: actual geographic coverage (verify a sample of the route list, don't take claims at face value), financial health (working capital relative to expected stock value), van sales team size and call frequency, cold-chain infrastructure for temperature-sensitive products (inspect the facility), existing portfolio conflicts with competing brands, and reputation with pharmacies in the territory. Weighting these before evaluation prevents selecting on coverage claims while missing operational capability gaps.
What stock cover level should a distributor maintain?
A widely adopted starting point is a floor of 21 days of cover (based on average daily offtake) with a ceiling of 45-60 days, these are recommended contract targets, not published industry benchmarks. Below the floor, the distributor should reorder automatically. Above the ceiling, both parties should investigate to prevent expiry risk. The right thresholds depend on your product's demand volatility, shelf life, and the logistics capability of your distributor. Specify them in the distribution agreement rather than assuming a shared understanding.
How should secondary-sales reporting be built into a distributor contract?
Define the reporting format, frequency (weekly or monthly), submission deadline, and data-sharing tool or template in the contract before the agreement is signed. Leaving secondary-sales reporting as an informal request creates ambiguity that distributors typically resolve in their favor when it's operationally inconvenient. Linking incentive payments to secondary-sales data quality and timeliness is one of the most effective enforcement mechanisms.
What is a reasonable fill rate target for a pharma distributor?
A commonly adopted target is 95% or above on orders fulfilled in full within the agreed lead time. Below 90% for two consecutive months is a widely used trigger for a formal performance review. These are recommended contractual benchmarks rather than published industry standards, your actual target should reflect your category, distributor tier, and market logistics. Fill rate tracks whether the distributor has adequate stock and operational capacity, not just whether they are willing to supply. A persistent miss usually indicates a structural problem with stock planning or financial working capital.
How do parallel imports harm pharma distributors?
Parallel imports bring product from a lower-price market into a higher-price market through unauthorized channels. This undercuts the authorized distributor's margin and weakens their commercial motivation to invest in your brands. Authorized distributors who see their territory undercut by parallel product will deprioritize your SKUs in favor of brands where they hold a more defensible commercial position. Detection through pack serialization and batch tracking, combined with supply restriction to the source market, is the standard mitigation.
When should a pharma company co-invest in a distributor's van sales team?
In high-potential territories where your portfolio's margin table doesn't naturally attract the distributor's best commercial energy, co-investing in dedicated van sales headcount aligned to your products can be justified. This is expensive but creates a salesforce operating under your commercial priorities rather than the distributor's broader portfolio incentives. The investment is typically warranted at product launch, during a market share campaign, or in territories where a competitor is actively building distributor relationships.
Learn More

Senior Implementation Consultant
On this page
- Distributor vs Stockist vs Wholesaler: Getting the Definitions Right
- Distributor Selection Criteria: What Actually Matters
- Onboarding and Contracting: Setting the Relationship Up Right
- Performance Scorecard: Measuring What Matters
- Incentive and Trade Terms Design
- Conflict and Escalation Management
- Distributor Relationships as a Strategic Asset
- Learn More