Pharma CRM and Sales Force Automation: The Commercial Backbone for Field Force Performance
Turn this article into takeaways for your work.
Each assistant summarizes the article only for you and suggests best practices for your work.
Most pharma customer relationship management (CRM) platforms start with big ambitions and end up as expensive contact databases. Reps enter call notes to satisfy compliance. Managers pull reports to satisfy regional directors. And commercial leadership stares at dashboards that show activity without explaining performance.
It doesn't have to work that way. When you deploy CRM and sales force automation (SFA) with the right architecture, governance, and change management, you get something genuinely powerful: a system reps use willingly because it makes their day easier, and leadership trusts completely because the data is clean and current.
This article gives pharma commercial leaders the framework to get there.
What Pharma CRM and SFA Actually Cover
Pharma CRM is not general-purpose B2B software with a life sciences skin painted on.
Key Facts: Pharma CRM Adoption
- A Deloitte survey of biopharma sales teams found that nearly 70% of reps said administrative work like post-meeting reports adds little to no value, pointing directly at CRM design failures that push data entry burden onto the field (Deloitte, 2026)
- Pharma CRM practitioners widely observe that field forces with lengthy manual call reports (10 or more fields) see measurably lower data completeness than those with streamlined five-or-fewer-field designs; the gap between the two approaches can be substantial enough to undermine coaching and forecasting reliability
- In the authors' assessment of the pharma field force landscape, most organizations operate at Stage 2 CRM maturity (structured activity tracking), with the commercial value of Stage 3 (integrated commercial intelligence with CLM and secondary sales feeds) requiring integration investments most have deferred
Pharma CRM is purpose-built for the specific operating context of a field force calling on healthcare professionals, pharmacies, hospitals, and drug stores. The core functions break down across five areas.
Health care professional (HCP) master data and segmentation records. Your CRM is the authoritative source for every HCP in your universe: specialty, prescribing tier, preferred call time, language preference, institutional affiliation. Segmentation data (A/B/C classification or decile ranking) determines who gets priority calls and how often. If this master data is wrong, every downstream decision built on it is also wrong.
Call activity logging and frequency tracking. Every rep visit generates a call report: who was visited, which products were detailed, what materials were presented, how many samples were left, and what the agreed next step is. SFA automates as much of this as possible so reps spend seconds, not minutes, completing each report. Frequency tracking compares actual call rates against target frequency by segment to surface coverage gaps before they become performance problems.
Sample management and e-signature compliance. Sample accountability is a regulatory requirement, not a nice-to-have. SFA handles sample request submissions, e-signature capture at point of delivery, balance tracking against rep allocation, and reconciliation reporting. Systems that get this wrong create audit exposure under the FDA's Prescription Drug Marketing Act, which mandates specific record-keeping for all sample distribution and prohibits the resale of samples.
Territory and account assignment workflows. When territories are realigned, when reps join or leave, or when HCP reclassifications happen, the CRM must update assignments automatically and maintain historical records. Manual territory updates are a data integrity risk.
Integration with CLM, ERP, and secondary sales feeds. A CRM that stands alone is a CRM that can't answer commercial questions. Integration with your closed-loop marketing (CLM) platform connects content engagement data to call records. ERP integration connects orders and inventory. Secondary sales feeds from distributors connect rep activity to actual sell-through, which is the outcome that matters. We cover how this comes together in the field reporting and closed-loop marketing article.
What Separates a Pharma CRM That Sticks from One That Gets Bypassed?
The Rep Experience First principle is the design rule that a pharma CRM should be architected from the field rep's daily workflow upward, not from the commercial dashboard downward. This means prioritizing offline capability, auto-population of routine fields, compliance guardrails that are invisible when reps follow policy, and a call report that takes under 60 seconds to complete, before investing in analytics layers or reporting features. CRM systems that skip this foundation generate abundant data that reps don't trust, managers don't use, and leaders discount.
Key Platform Capabilities to Evaluate
When selecting or upgrading a pharma CRM platform, evaluate these four capability areas above product brand or vendor relationships.
Offline-First Mobile Architecture
Your reps call on clinics in basements, hospitals in elevator dead zones, and rural pharmacies with no signal. A CRM that requires connectivity to function is a CRM that gets bypassed in the field and batch-updated at the end of the day, which means data is 8 hours old by the time it's recorded.
Offline-first means the full app functions without a connection: viewing HCP profiles, logging calls, capturing e-signatures, and submitting sample requests. Sync happens automatically when connectivity is restored. This is non-negotiable for any field force operating outside dense urban areas.
Auto-Population to Reduce Admin Burden
The single biggest driver of CRM abandonment is rep perception that data entry benefits compliance rather than them. Every field you auto-populate from existing data is a field reps don't have to touch. Good SFA platforms pull in the HCP's name, last visit date, current sample balance, and most recent CLM engagement score automatically when a rep opens a call report. The rep confirms, edits if needed, and submits in under 60 seconds.
Review your current call report template and count the fields. Anything above 10 manual fields is driving abandonment. Target 5 or fewer fields that require rep input; everything else should come from the system.
Compliance Guardrails Built Into the Workflow
Compliance controls should be invisible when reps are operating within policy, and impossible to bypass when they're not. That means:
- Sample limits enforced at point of request (rep can't over-distribute)
- Blacklisted HCPs flagged before a call is logged, not after
- Fair balance reminders triggered automatically when product benefits are entered without risk information
- Signature capture required before samples leave the rep's trunk
Compliance that exists only in training decks gets violated. Compliance built into the system workflow doesn't.
Configurable HCP Universe and Targeting Alignment
Your targeting model changes. New product launches, seasonal adjustments, market access shifts, and competitive moves all require updates to who reps should call and how often. A CRM that requires IT involvement to update segmentation is too slow. Commercial ops should be able to update HCP tiers, frequency targets, and territory-level call plans without a development ticket.
CRM Capability Comparison: What Separates Good from Great
| Capability | Basic | Intermediate | Advanced |
|---|---|---|---|
| Call logging | Manual text entry | Structured dropdown fields | Auto-populated from HCP profile |
| Offline access | Requires connectivity | Read-only offline | Full offline functionality |
| Sample management | Manual tracking | In-app tracking, manual signature | E-signature with auto-reconciliation |
| Compliance controls | Training-based | Post-submission alerts | Workflow-embedded prevention |
| Segmentation updates | IT-dependent | Admin interface | Commercial ops self-service |
| CLM integration | None | Manual data export | Bi-directional real-time sync |
| Analytics | Activity counts | Coverage reports | Predictive call prioritization |
Common Deployment Failures and Their Root Causes
Most CRM implementations that underdeliver share the same failure patterns. Understanding them before you deploy saves you from learning them the hard way.
 Failure 1: Data entry as burden rather than benefit. When reps see call reporting as something done for compliance rather than something that makes their work easier, adoption suffers. The fix isn't more training. It's redesigning the call report so reps actually get something back from the data they enter: their call history, their next best action recommendation, their progress against call targets. If the only person who benefits from a rep's data entry is the compliance team, you've designed the system backwards. A Deloitte survey of biopharma sales teams found that nearly 70% of reps said administrative work like post-meeting reports adds little to no value, pointing directly at this design failure.
Failure 1: Data entry as burden rather than benefit. When reps see call reporting as something done for compliance rather than something that makes their work easier, adoption suffers. The fix isn't more training. It's redesigning the call report so reps actually get something back from the data they enter: their call history, their next best action recommendation, their progress against call targets. If the only person who benefits from a rep's data entry is the compliance team, you've designed the system backwards. A Deloitte survey of biopharma sales teams found that nearly 70% of reps said administrative work like post-meeting reports adds little to no value, pointing directly at this design failure.
Failure 2: Disconnected systems creating data silos. A CRM that doesn't talk to CLM creates a situation where marketing knows what content was shown and sales knows who was visited, but nobody knows both at once. A CRM that doesn't receive secondary sales data means reps can't see whether their calls are moving inventory. Integration is a commercial precondition, not an IT project to do later. See how Territory Analytics and Sales Dashboards depend on this integration.
Failure 3: Poor adoption from inadequate change management. CRM rollouts that treat training as a one-day event before go-live consistently underperform. Adoption requires sustained reinforcement: manager coaching that references CRM data in every field visit review, rep incentives tied to data quality, and visible leadership use of CRM outputs in commercial reviews. And if managers aren't using the system in their coaching conversations, reps won't use it either. A structured CRM adoption operating model is what converts a one-time launch into a sustained behavioral change across the field force.
The CRM Maturity Model: Four Stages
| Stage | Characteristics | What Changes |
|---|---|---|
| Stage 1: Basic Logging | Manual call reports, spreadsheet-level data, no integration. Compliance focus only. | CRM adoption measured by volume, not quality |
| Stage 2: Structured Activity Tracking | Standardized call report fields, frequency targets by segment, basic coverage reporting. Sales managers start using dashboards. | Coverage gaps visible, coaching conversations begin |
| Stage 3: Integrated Commercial Intelligence | CLM connected, secondary sales feeds active, HCP segmentation driven by prescribing data. Marketing and sales sharing data. | Next best action recommendations appear, territory optimization possible |
| Stage 4: Predictive Field Intelligence | AI-driven call prioritization, real-time alerting on coverage gaps, prescribing trend anomaly detection. | Rep time allocated by system-generated priority, not instinct |
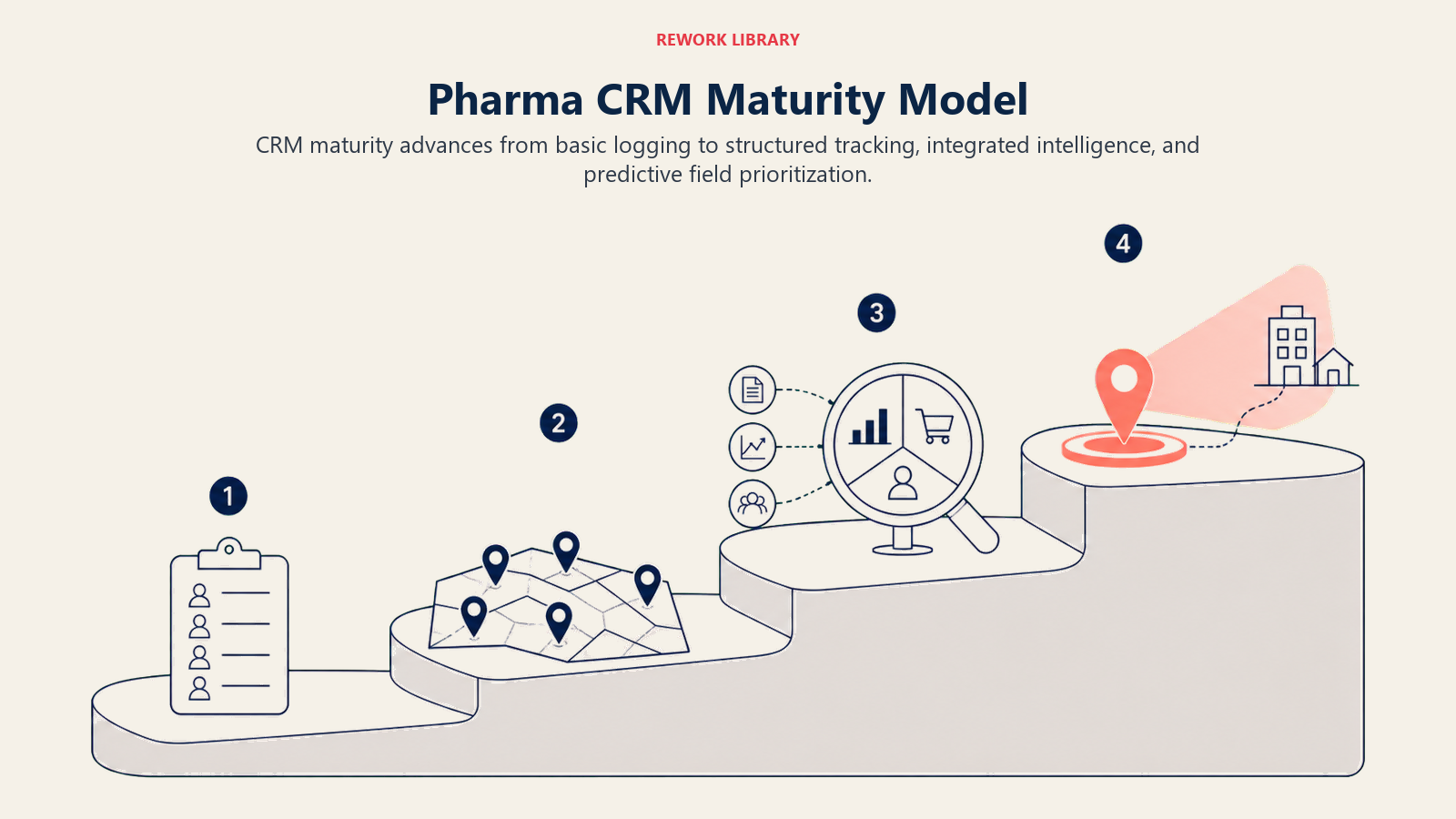 Based on what commercial teams report in practice, the majority of pharma field forces sit at Stage 2. Getting to Stage 3 requires the integration investments that many organizations defer. Stage 4 requires data volume and cleanliness that most organizations don't yet have. The focus for most commercial leadership teams should be closing the gap between Stage 2 and Stage 3.
Based on what commercial teams report in practice, the majority of pharma field forces sit at Stage 2. Getting to Stage 3 requires the integration investments that many organizations defer. Stage 4 requires data volume and cleanliness that most organizations don't yet have. The focus for most commercial leadership teams should be closing the gap between Stage 2 and Stage 3.
Integration Architecture: Connecting the Commercial Stack
A pharma CRM doesn't operate in isolation. It's the central hub that connects field activity to commercial intelligence, but that hub only works when the spokes are properly attached.
CRM to CLM integration means content shown during a rep visit (slides, video, survey responses) flows into the call record automatically. The rep doesn't re-enter what the HCP saw. Marketing gets engagement data tied to specific visits and HCPs. This is the foundation of closed-loop marketing.
CRM to ERP integration connects sample distribution in the field to inventory reconciliation in the warehouse. Sample requests submitted in CRM trigger ERP transactions. Balance updates sync back to rep devices. Audit trails exist on both sides.
CRM to secondary sales feed integration means territory-level sell-in and sell-out data from distributors appears in the same view as rep call activity. When a rep calls on 20 pharmacies this week and secondary sales are flat, the system surfaces that gap. Without integration, the rep and their manager are looking at disconnected data sets and having unproductive conversations about causation.
CRM to analytics dashboard integration means that the call frequency and coverage optimization models your sales ops team builds don't require manual data pulls. The CRM feeds analytics in near real-time, so dashboard data reflects what happened today, not what happened last week.
Governance and Data Quality
A CRM with dirty data is worse than no CRM, because bad data creates false confidence in decisions. Governance isn't glamorous, but it's what separates CRM systems that commercial leaders trust from those they quietly ignore.
Master data stewardship requires a dedicated owner, not a committee. One team (typically sales ops or commercial ops) is accountable for HCP master data quality: duplicate resolution, specialty updates, address verification, and blacklist management. That team sets the cadence for master data reviews (monthly at minimum) and owns the escalation path when data quality issues are flagged. The OIG Compliance Program Guidance for pharmaceutical manufacturers identifies data integrity and accurate reporting to government agencies as a primary risk area, which means the stewardship model for HCP master data has compliance and legal weight beyond its commercial utility. The operating principles for running this kind of stewardship program mirror the CRM data hygiene practices that revenue operations teams use in non-pharma businesses: the same duplicate-resolution logic, the same completeness scoring, and the same ownership model.
Duplicate HCP record prevention is easier to prevent than fix. Implement duplicate detection at record creation, not as a periodic cleanup. A rep who creates a duplicate HCP record because they can't find the existing one is a rep whose call history is now split across two records.
Territory sync cadence should align with your operational calendar. If territory realignments happen quarterly, CRM territory assignments should update before the quarter begins, not during it. Mid-quarter updates create attribution gaps where calls fall into neither old nor new territory assignments.
Data completeness monitoring means tracking the percentage of call reports with all required fields completed, the percentage of HCPs in the universe with current segmentation data, and the percentage of sample transactions with completed e-signatures. These metrics belong in the same review that commercial leaders use for sales performance.
ROI Framework: Measuring CRM Value
CRM investments are justified by commercial outcomes, not adoption metrics. Here are the metrics that tell you whether your CRM is working.
Call plan adherence rate. The percentage of target calls completed versus planned, broken down by segment tier. A rep hitting 90% adherence for Tier A HCPs and 40% for Tier B is making prioritization decisions in the field that may or may not align with commercial strategy. This metric makes those decisions visible.
HCP coverage rate. The percentage of the target HCP universe reached at least once per cycle. Low coverage often indicates territory design problems (too many HCPs per rep) or time management problems (too much time in high-frequency accounts, not enough breadth).
Data completeness score. The percentage of call reports fully completed within 24 hours of the visit, with all required fields populated. Scores below 85% indicate adoption problems. Scores below 70% indicate a system problem, not just a behavior problem.
CRM-to-prescription correlation. For regions with access to prescribing data, the correlation between CRM call frequency for a given HCP and that HCP's prescribing trend for your products. This is the metric that connects CRM activity to commercial outcomes and justifies the investment to CFOs who view CRM as a cost center.
These metrics integrate into broader sales ops and field force alignment frameworks and feed the data reps use to structure their medical rep daily call plan.
Building a CRM Reps Use Willingly and Leadership Trusts Completely
The CRM that succeeds in pharma field force management does two things simultaneously: it makes the rep's job easier in the field, and it gives commercial leadership the data quality and analytical depth to make confident decisions.
Those two goals aren't in tension. They're the same goal approached from different ends. When reps trust that the system works for them, they enter accurate data. When data is accurate, analytics are reliable. When analytics are reliable, leadership makes better decisions. When decisions are better, targets get hit, and the cycle reinforces itself.
The organizations that get this right start with the rep experience and work up, not with the dashboard and work down. They invest in offline capability, auto-population, and compliance-embedded guardrails before they invest in analytics layers. They build data quality governance before they build predictive models. And they make sure every manager uses CRM data in their coaching conversations before they launch new reporting features.
That sequence matters. A pharma CRM is only as valuable as the data inside it, and the data is only as good as the reps' willingness to enter it accurately and promptly. Get that right, and the analytics, coaching, and forecasting capabilities you invest in on top will actually work.
Frequently Asked Questions about Pharma CRM and Sales Force Automation
What is the difference between pharma CRM and sales force automation?
CRM (customer relationship management) refers to the master data layer: HCP profiles, segmentation, account history, relationship records, and call logs. Sales force automation (SFA) refers to the workflow tools that operate on that data: call report submission, sample management, route planning, and frequency tracking. In practice, most pharma platforms bundle both. Veeva CRM and IQVIA OCE, the two dominant platforms in life sciences, provide integrated CRM plus SFA in a single mobile-first application.
How many fields should a pharma call report contain?
Five or fewer fields that require active rep input. Everything else should be auto-populated from the HCP record (name, last visit date, segmentation tier), the CLM platform (materials shown, time per slide), or the sample management system (quantities distributed, e-signature status). Pharma CRM practitioners consistently observe that lengthy reports with 10 or more manual fields drive lower completeness and higher abandonment than streamlined designs that auto-populate most fields and require reps to confirm rather than type.
What does offline-first mean for a pharma CRM?
Offline-first means the full application functions without an internet connection: viewing HCP profiles, logging calls, capturing e-signatures, and submitting sample requests. Data syncs automatically when connectivity is restored. This is non-negotiable for any field force that calls on hospital basements, rural pharmacies, or clinic buildings with poor signal. A CRM that requires connectivity to function gets bypassed in the field and batch-updated at the end of the day, producing data that's 8 hours old by the time it's recorded.
How should HCP master data be governed in a pharma CRM?
One team, typically sales operations or commercial operations, should own HCP master data quality with clear accountability for duplicate resolution, specialty updates, address verification, and blacklist management. Governance by committee without a designated owner produces gaps. Master data reviews should run at least monthly. Duplicate detection at record creation is far cheaper than periodic deduplication cleanup: a rep who creates a duplicate HCP record splits the call history across two records and corrupts both frequency tracking and outcome analytics.
What is CRM-to-prescription correlation and why does it matter?
CRM-to-prescription correlation measures the relationship between call frequency for a given HCP in the CRM and that HCP's prescribing trend for the rep's products, using external prescribing audit data from sources like IQVIA or MIMS. This metric is the commercial proof point that connects field activity investment to outcomes. Without it, CRM analytics answer only "what did reps do?" With it, they can answer "does what reps do actually move prescribing?" That distinction matters for every budget conversation about field force headcount and call frequency targets.
When is the right time to upgrade from Stage 2 to Stage 3 CRM maturity?
Stage 3 maturity, which adds CLM integration, secondary sales feeds, and HCP segmentation driven by prescribing data, is appropriate when CRM call logging is consistent (completeness rates above 85%), basic coverage and frequency reporting is trusted and used by managers in coaching conversations, and there is commercial leadership commitment to act on the integrated data rather than just reporting on it. Organizations that invest in Stage 3 analytics before their Stage 2 data quality is solid end up with sophisticated dashboards built on unreliable foundations.
Learn More

Senior Implementation Consultant
On this page
- What Pharma CRM and SFA Actually Cover
- What Separates a Pharma CRM That Sticks from One That Gets Bypassed?
- Key Platform Capabilities to Evaluate
- Offline-First Mobile Architecture
- Auto-Population to Reduce Admin Burden
- Compliance Guardrails Built Into the Workflow
- Configurable HCP Universe and Targeting Alignment
- CRM Capability Comparison: What Separates Good from Great
- Common Deployment Failures and Their Root Causes
- The CRM Maturity Model: Four Stages
- Integration Architecture: Connecting the Commercial Stack
- Governance and Data Quality
- ROI Framework: Measuring CRM Value
- Building a CRM Reps Use Willingly and Leadership Trusts Completely
- Learn More