Pharmaceutical Sales Growth Model: The Field-Force Framework for Commercial Leaders
 Most pharma field forces don't have a growth model. They have a headcount plan and a list of targets.
Reps visit doctors. Other reps cover pharmacies. A hospital team chases tenders. Marketing runs campaigns in parallel. Nobody has a clear view of how all that activity connects to prescription volume, secondary sales, or market share growth. When numbers fall short, the instinct is to add reps or cut territories, not to diagnose the system.
Most pharma field forces don't have a growth model. They have a headcount plan and a list of targets.
Reps visit doctors. Other reps cover pharmacies. A hospital team chases tenders. Marketing runs campaigns in parallel. Nobody has a clear view of how all that activity connects to prescription volume, secondary sales, or market share growth. When numbers fall short, the instinct is to add reps or cut territories, not to diagnose the system.
Turn this article into takeaways for your work.
Each assistant summarizes the article only for you and suggests best practices for your work.
That's the fragmentation problem. It's why so many field forces plateau. They're executing disconnected tactics rather than running an integrated commercial operation. The solution is a growth model. Not a strategy deck, not a KPI dashboard. An actual operating framework that explains how field activity converts to revenue, where the pressure points are, and what needs to happen at each customer touchpoint for growth to compound.
This article lays out that framework for pharma commercial leaders. It covers the five core growth levers, the three customer universes your field force must serve, the growth flywheel that ties them together, and how to apply the model depending on where your brand is in its lifecycle.
The Five Levers of Pharma Commercial Growth
Pharma growth doesn't come from one place. It comes from five interconnected levers working in sequence. Pull on only one and you get a short spike. Pull on all five in the right order and you build compounding momentum. The ADFEL Model (Access, Demand, Field Execution, Loyalty, channel pul[L]-through) is the shorthand for this sequencing: each letter maps to a lever, and the order is deliberate. Access before Demand, Demand before Field Execution at scale, pull-through alongside execution, and Loyalty as the compounding layer on top.

Lever 1: Market Access
Before a rep can drive a single prescription, someone has to be allowed to prescribe and dispense your product. Market access is the foundation of the model. It covers formulary listings in hospitals and clinics, reimbursement status with national and regional health schemes, distribution agreements with wholesalers and pharmacy chains, and tender wins in institutional channels. In lower-income markets, WHO essential medicines data shows medicines can account for 20 to 60% of health spending, making reimbursement access a defining commercial constraint.
Without market access, field effort is wasted. A rep who details a doctor on a drug that isn't covered or stocked is generating awareness, not revenue. Market access has to come first, and field leadership needs to know exactly where access gaps exist before deploying coverage resources.
Lever 2: Demand Generation
Demand generation is how HCPs (healthcare professionals, including doctors, specialists, and clinical pharmacists) learn about your product, develop confidence in it, and begin recommending it to patients. This is the traditional domain of medical rep detailing, scientific education, key opinion leader (KOL) engagement, CME sponsorships, and clinical symposia.
The output of demand generation isn't a sale. It's a shift in prescribing behavior. Measuring it requires tracking awareness scores, prescribing intent, new-to-brand (NtB) scripts, and share-of-voice among targeted HCPs. If demand generation is working, prescription rates rise before secondary sales data catches up. If it's stagnating, your reps are getting face time without changing minds.
Lever 3: Field Execution
Field execution is the operational heartbeat of the model. It covers rep visit frequency, call quality and detail delivery, sampling programs, coverage of the right account universe, and CRM compliance. Understanding the pharma field sales economics behind each visit type is essential here. A doctor call costs differently than a pharmacy visit or a hospital account review, and the revenue return varies considerably.
Strong field execution doesn't mean visiting every possible target. It means visiting the right targets at the right frequency with the right message. A rep spending 60% of their time on low-prescribing doctors is executing calls, not driving growth. Field execution quality is ultimately measured by the pharmaceutical sales KPIs and metrics that track whether visits translate into behavioral change.
Lever 4: Channel Pull-Through
Demand from HCPs only converts to revenue if the product is available where patients try to fill their prescriptions. Channel pull-through is the link between prescribing intent and actual dispensing, and it's where many field forces lose significant revenue.
Pull-through work includes ensuring pharmacies carry adequate stock, monitoring out-of-stock events, maintaining shelf presence in key outlets, and educating pharmacy staff on dispensing protocols and substitution handling. It also means tracking the gap between prescriptions written (primary sales proxy) and units actually dispensed (secondary sales), which is the real commercial outcome. IQVIA prescription tracking covers 87 countries and 709 therapeutic classes, making it the standard data source for this gap analysis across most commercial markets.
Lever 5: Loyalty and Retention
The most expensive customer is the one you have to re-convince every quarter. Loyalty and retention work builds on established prescribing relationships to deepen advocacy, defend against competitor switching, and expand prescribing breadth (getting doctors to prescribe your product for a wider range of patient profiles).
In pharmacy channels, loyalty looks like preferred shelf placement, consistent ordering behavior, and pharmacy staff who proactively recommend your product when substitution is available. With HCPs, it looks like repeat prescribing, unprompted recommendation to colleagues, and willingness to speak on your behalf at peer events.
Key Facts: Pharma Commercial Scale
- The global pharmaceutical market reached close to $1.7 trillion in annual revenues in 2024, per Statista industry data.
- IQVIA prescription tracking covers 87 countries and 709 therapeutic classes, making it the standard benchmark for sell-out gap analysis across most commercial markets.
- WHO essential medicines data shows medicines account for 20 to 60% of health spending in lower-income markets, making reimbursement access a defining commercial constraint.
Three Customer Universes
The five levers play out differently across three distinct customer types. Your field force almost certainly covers all three, but the way you engage each one, and the revenue cycle each feeds, is fundamentally different. Universe 1: Pharmacies and Drug Stores
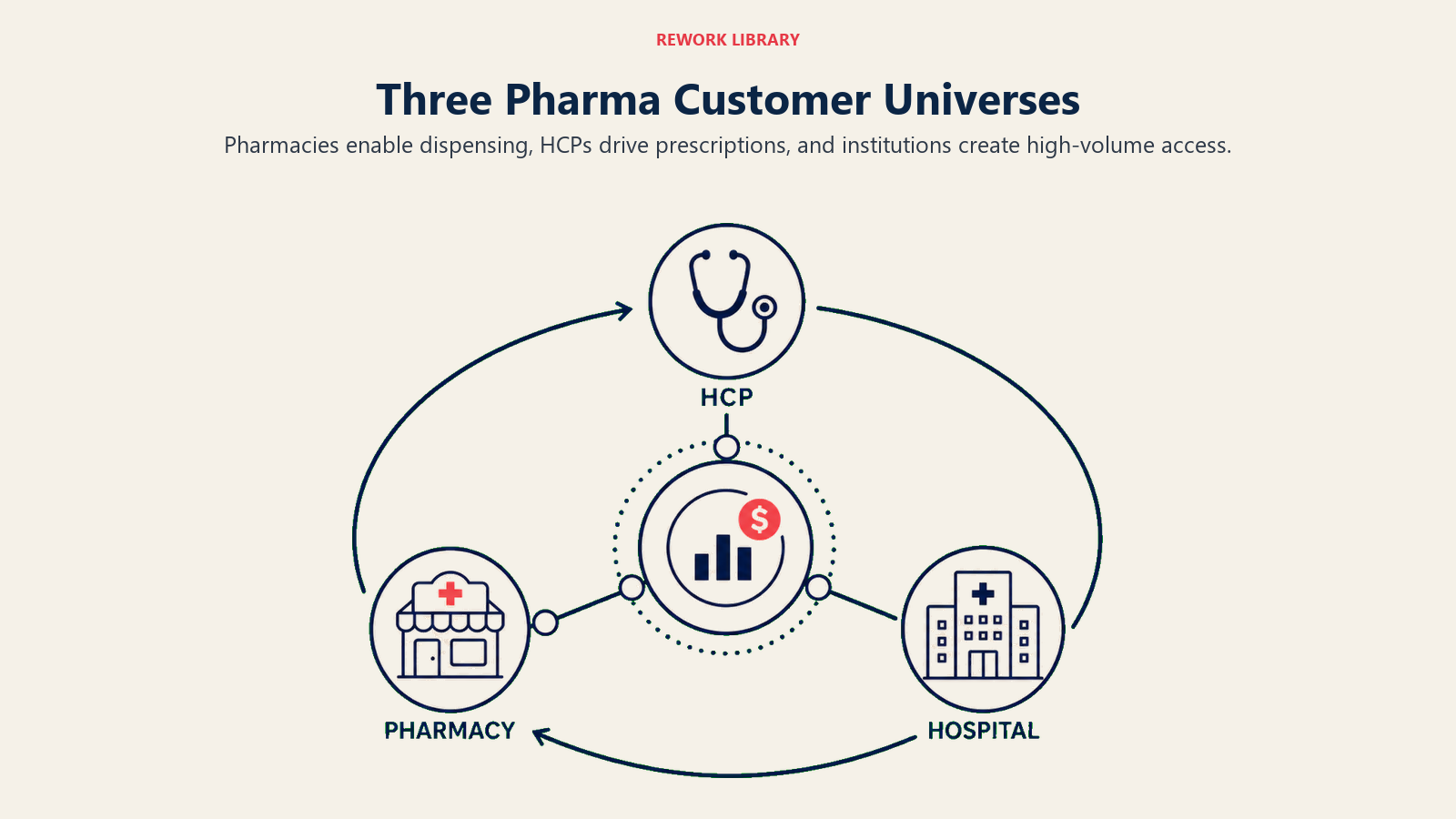
Pharmacies sit at the last mile of the prescription journey. Their primary commercial role is availability and dispensing. A pharmacy that runs out of stock, substitutes a competitor product, or doesn't stock your SKU at all kills revenue that demand generation already created.
The field objective in this channel is pull-through: stock compliance, ordering regularity, and pharmacist education. The commercial relationship is built through pharmacy reps or trade sales teams who focus on sell-out (what actually leaves the shelf) rather than sell-in (what's been invoiced to the pharmacy). Sell-in without sell-out creates channel inventory bloat and distorts your sales picture.
Pharmacies also play a soft advocacy role. When a doctor writes a generic prescription or a patient asks for a recommendation, the pharmacist's default choice matters. Field activity here includes detailing clinical benefits to dispensing staff and providing educational materials that shape those day-to-day decisions.
Universe 2: Doctors and HCPs
Doctors and specialists are the primary prescription drivers. In most markets, a prescribing decision by a physician or specialist represents significant downstream revenue, so the ROI on HCP detailing is high for the right targets.
Effective HCP engagement requires customer segmentation and targeting built on prescribing data, not just geography. Defining the right HCP profile before deploying coverage is essential: without a clear picture of who the highest-value targets are, field effort disperses into low-return contacts. The same principle that governs lead scoring systems in B2B sales applies here: assign weighted scores to account potential and behavioral signals, then let the model determine call priority rather than relying on geography or intuition alone. A doctor who sees 200 patients per month in your therapeutic area is a fundamentally different investment than one who sees 20. Targeting compliance (are your reps actually visiting the right doctors?) is one of the most important operational metrics in this channel.
The field model for HCPs is relationship-plus-evidence. Reps build personal relationships that create access, then use scientific evidence, sampling, and clinical data to influence prescribing behavior. KOLs play an amplifying role: a senior specialist who publicly endorses your product creates peer-level credibility that no rep visit can replicate.
Universe 3: Hospitals and Institutions
Hospital selling is structurally different from retail or primary care. Purchasing decisions are made collectively by pharmacy and therapeutics committees, medical directors, and procurement teams. Individual doctor advocacy matters, but it has to translate into formulary inclusion or tender wins to generate revenue.
Hospital accounts generate high volume per account but require longer sales cycles, tender management expertise, and a separate account relationship model. A hospital account manager who excels at committee navigation and institutional negotiation is a different profile from a primary care rep who builds one-to-one doctor relationships.
The revenue cycle from hospital activity is also different: formulary listings create recurring high-volume purchases, and losing a hospital tender can cost more revenue in one quarter than losing dozens of individual prescribers.
The Growth Flywheel
These three customer universes don't operate in isolation. They form a flywheel that, when running correctly, creates self-reinforcing commercial momentum. KOL advocacy among specialists builds credibility with general practitioners, who begin prescribing more frequently. Rising prescription volumes create pull-through demand at pharmacies, which generates sell-out data that confirms market share growth. That commercial success funds continued field investment, which strengthens the KOL program, which amplifies specialist advocacy, and the cycle continues. Momentum builds when each stage of the cycle reinforces the next, and stalls when any single handoff breaks. The alignment between marketing and field sales is essential to keeping this flywheel spinning. Marketing campaigns that build HCP awareness need field execution to convert that awareness into prescribing. Field activity that creates pharmacy demand needs supply chain and trade support to prevent out-of-stock events that break the cycle.
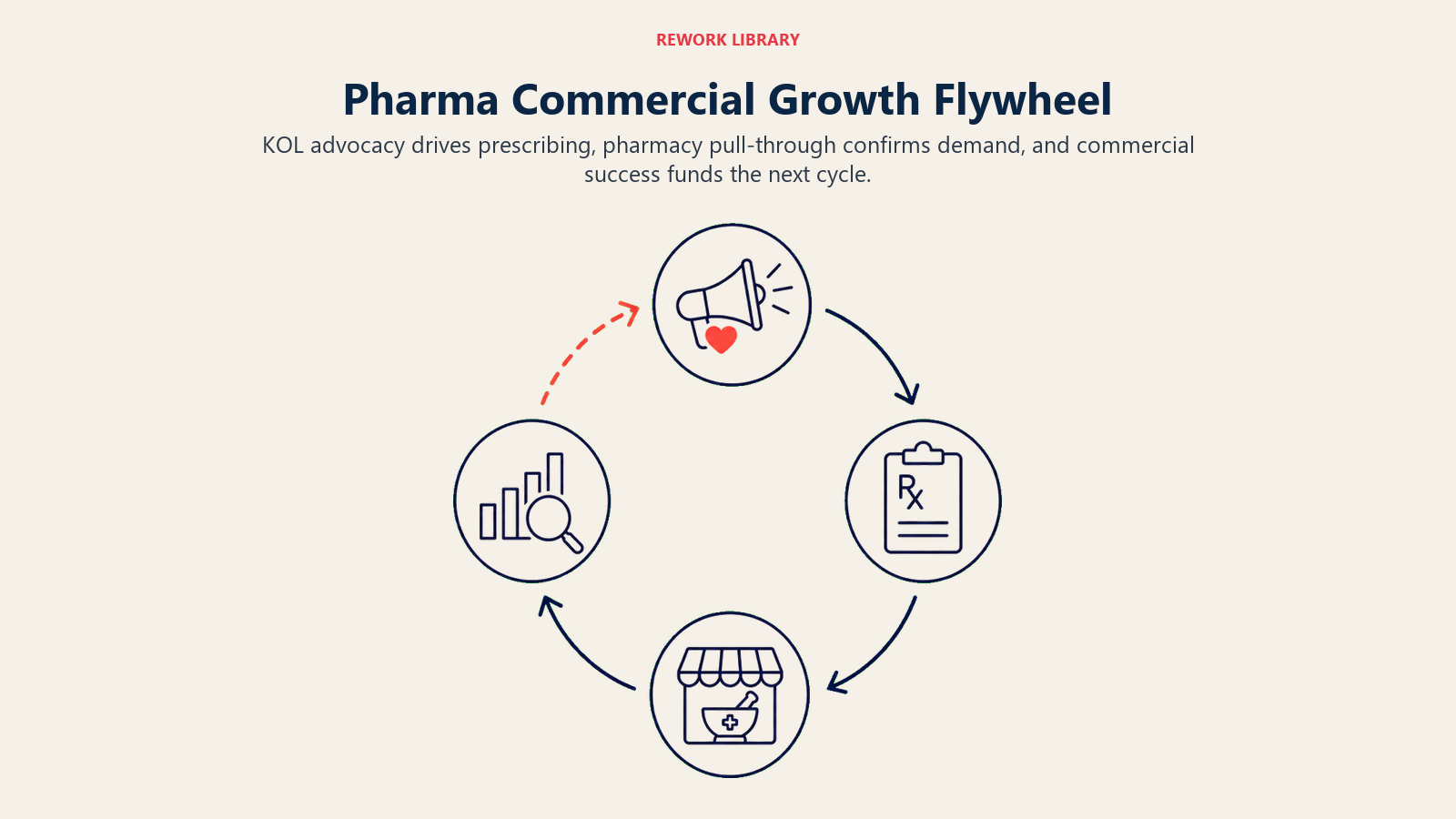
When the flywheel breaks, it usually breaks at one of three points: HCPs are aware but not converting to scripts (a detailing quality problem), pharmacies are stocked but dispensing the wrong product (a pull-through execution problem), or market access gaps mean prescriptions can't be filled (a coverage problem). Understanding which handoff is broken is the first step toward knowing where to apply pressure.
Where Do Field Forces Break Down?
Field force underperformance rarely comes from one broken lever in isolation. It comes from sequencing errors: investing in Lever 3 (field execution) before Lever 1 (market access) is complete, or scaling headcount before Lever 2 (demand generation) has created the HCP awareness that makes visits productive. Companies that skip the sequencing discipline waste significant field spend on activity that cannot convert to revenue regardless of rep quality or call frequency.
The growth model makes it easy to see where failure actually originates, rather than treating underperformance as a generalized "sales problem."
Coverage gaps in high-value segments: Reps visiting the wrong targets, or not visiting high-potential accounts at a sufficient frequency. This is a sales territory mapping problem that compounds over time as competitors capture prescribers you've deprioritized.
Misaligned incentives between demand and pull-through: Reps compensated purely on primary sales (sell-in) have no incentive to manage pharmacy pull-through. If their numbers look good but secondary sales are lagging, they're building channel inventory rather than market share.
Poor pull-through measurement: Many commercial teams can tell you what they sold in, but not what actually sold out. Without secondary sales data, you can't see where demand is leaking after the prescription is written.
Disconnected hospital activity: Hospital team wins formulary inclusion but doesn't coordinate with primary care reps to drive HCP referrals or with pharmacy teams to ensure stock availability. The institutional win doesn't flow through to the broader commercial system.
Weak KOL activation: KOL relationships exist but aren't systematically used to influence peer prescribing. The flywheel stalls because the advocacy signal never reaches the mass of prescribers who follow KOL leadership.
Applying the Model by Maturity Stage
The five levers don't get equal weight at every point in a brand's lifecycle. How you allocate field effort and where you focus commercial investment shifts as the brand matures. | Stage | Primary Focus | Secondary Focus | Field Priority | |---|---|---|---| | Launch | Market access, demand generation | Field execution coverage | Formulary listings, KOL activation, NtB scripts | | Growth | Demand expansion, pull-through | Loyalty, frequency optimization | Targeting compliance, pharmacy stocking, prescriber breadth | | Maturity | Loyalty, competitive defense | Channel efficiency | Defending key prescribers, secondary sales, cost-per-call optimization | | Decline | Retention, niche defense | Channel rationalization | High-value account focus, reduced field footprint |
At launch, access gaps and awareness gaps are the limiting factors. Market access work and KOL activation come before mass rep detailing because reps can't drive scripts on a product that isn't covered or credible yet.
In the growth stage, the constraint shifts to execution. You have access and awareness; now the question is whether your field force is systematically converting that into prescribing behavior and pharmacy availability at sufficient scale.
At maturity, the game is defense and efficiency. You're protecting prescriber relationships from competitive switching while managing your cost-per-call to maintain acceptable field ROI. The field force audit below helps you locate exactly where your organization sits against each lever.
Field Force Audit Against This Framework
Use this checklist to assess where your field force sits against the growth model: Market Access
- Do you have formulary listings in all target hospitals?
- What percentage of your target patient population has reimbursement access?
- Are there distribution gaps in key pharmacy chains?
Demand Generation
- What is your share of voice among target HCPs versus key competitors?
- What percentage of your target prescribers have received a detail in the last 90 days?
- What is your new-to-brand script rate among first-time prescribers?
Field Execution
- Is targeting compliance above 70% (reps visiting priority A/B accounts at target frequency)?
- What is your average call quality score across your field force?
- Are sampling programs generating measurable script conversion?
Pull-Through
- What is the gap between primary and secondary sales in your top markets?
- What is the out-of-stock rate in key pharmacy chains?
- Are pharmacy reps covering high-volume pharmacies at the right frequency?
Loyalty and Retention
- What is your prescriber retention rate (doctors who prescribed last quarter still prescribing)?
- What is your pharmacy repeat order rate?
- Are KOLs actively engaged in peer education programs?
If you have gaps in the first two pillars (access and demand), adding field headcount won't accelerate growth. Fix the access and advocacy foundation first, then scale execution. That sequencing is the difference between a field force that performs and one that churns through activity without compounding results.
Frequently Asked Questions about Pharmaceutical Sales Growth Model
What is a pharma commercial growth model?
A pharma commercial growth model is an operating framework that explains how field activity converts to revenue across the full customer chain, from market access through to pharmacy dispensing. It differs from a strategy deck or KPI dashboard because it specifies the sequence of levers (access, demand, execution, pull-through, loyalty) and shows where in that sequence growth is being created or lost.
Why do most pharma field forces plateau instead of compound?
Most field forces plateau because they're executing disconnected tactics rather than running an integrated system. Reps visit doctors, other teams cover pharmacies, and hospital teams chase tenders, but without a clear model connecting those activities to revenue, underperformance gets treated as a headcount problem rather than a sequencing or alignment problem. The growth model exposes the actual constraint.
What is the most common lever pharma companies missequence?
Companies most often scale field execution (Lever 3) before market access and demand generation (Levers 1 and 2) are established. Adding rep headcount when formulary coverage is incomplete or when HCP awareness is too low means reps are generating activity that cannot convert to prescriptions, regardless of call quality or frequency. Fix access and advocacy first, then scale execution.
What is the difference between primary sales and secondary sales in pharma?
Primary sales refers to units sold into distribution channels (sell-in), meaning product invoiced to wholesalers or pharmacies. Secondary sales refers to units actually dispensed to patients (sell-out). The gap between these two numbers is a critical commercial signal: a large sell-in-to-sell-out gap indicates channel inventory loading, not real patient demand, and often corrects sharply when the channel destocks.
How does the pharma growth flywheel work?
The flywheel works through reinforcing cycles across the three customer universes. KOL advocacy among specialists builds credibility with GPs, who begin prescribing more frequently. Rising prescriptions create pull-through demand at pharmacies, which generates sell-out data confirming market share growth. That commercial success funds continued field investment, which strengthens KOL engagement, and the cycle continues. Any break in the handoffs between stages stalls the flywheel.
How does brand lifecycle stage change which levers to prioritize?
At launch, market access and demand generation are the binding constraints: formulary listings and KOL activation come before mass rep detailing. In the growth stage, field execution and pull-through become the primary levers, converting existing awareness into prescribing scale. At maturity, loyalty and competitive defense take priority, protecting the prescriber base while managing field cost efficiency. Misapplying launch-stage resource allocation to a mature brand wastes investment on awareness that already exists.
What should a field force audit check first?
Start with market access coverage: the percentage of target patients who have reimbursement access to your product, and the formulary listing rate across target hospitals. If access gaps are material, no amount of detailing investment will unlock the full revenue potential of the territory. Only after confirming access is complete does it make sense to audit execution quality, targeting compliance, and pull-through performance.
Learn More
