HCP Relationship Retention: Keeping Prescribers Engaged After the First Script
Turn this article into takeaways for your work.
Each assistant summarizes the article only for you and suggests best practices for your work.
A doctor who wrote one prescription last quarter is not a loyal prescriber. They're a trialist. And the gap between a trialist and an ongoing advocate is where most pharma field forces lose more market share than any competitor launch ever takes from them.
Acquisition gets the attention. New HCP (health care professional) targets, expanded coverage lists, first detailing visits: these are the metrics that show up in launch planning and territory target-setting. But retention, the discipline of keeping prescribers engaged after the first script, is where the commercial value actually accumulates. A doctor who prescribes consistently over three years is worth exponentially more than a doctor who tried the product once and drifted back to their default choice.
The field forces that build durable prescribing relationships don't do it through relationship instinct or rep charisma. They do it through structured retention disciplines: defined visit agendas, segmented strategies by prescriber type, clinical value delivery that makes the doctor better at their job, and early warning systems for detecting competitive erosion before it shows up in prescription data.
HCP Retention vs HCP Acquisition: Different Disciplines
This distinction matters operationally, not just conceptually. The tactics, the conversation types, the KPIs, and even the rep skills required for retention work are different from acquisition.
Acquisition is about generating trial. The first detailing visit focuses on the product's efficacy profile, safety data, and positioning against the current standard of care. Success is measured by whether the doctor tries the product with an appropriate patient.
Retention is about deepening clinical confidence and broadening prescribing patterns. The ongoing visit focuses on how the doctor's experience with the product has translated to patient outcomes, which patient types are responding well, what questions have emerged from actual clinical use, and what clinical evidence or peer insights can help them prescribe more effectively.
A rep who runs the same acquisition-style detail on the fifth visit that they used on the first is not running a retention program. They're re-pitching to a prescriber who already decided to try the product. That approach erodes rather than builds prescribing confidence. Research confirms that pharmaceutical rep visits remain a primary drug information source for many physician practices, which makes the quality and relevance of each visit more consequential than frequency alone.
Key Facts: HCP Relationship Retention
- Rep visit quality matters more than visit frequency: physician practices rank pharmaceutical rep visits as a primary drug information source, meaning a poorly prepared retention visit can do more harm than a missed one.
- A pilot study of rare disease prescribers (34 respondents, UK) found that non-promotional personal engagement may be more influential on prescribing decisions than standard promotional rep activity, reinforcing the value of escalating complex clinical questions to the MSL team rather than attempting to answer them at the rep level.
- Illustrative target benchmarks for field force retention programs typically aim for greater than 80% quarter-on-quarter retention among top-tier prescribers and lapsed prescriber reactivation rates above 30% within 90 days of a structured reactivation visit; your organization should calibrate these thresholds against your own therapeutic area and territory data.
Segmenting Retained HCPs
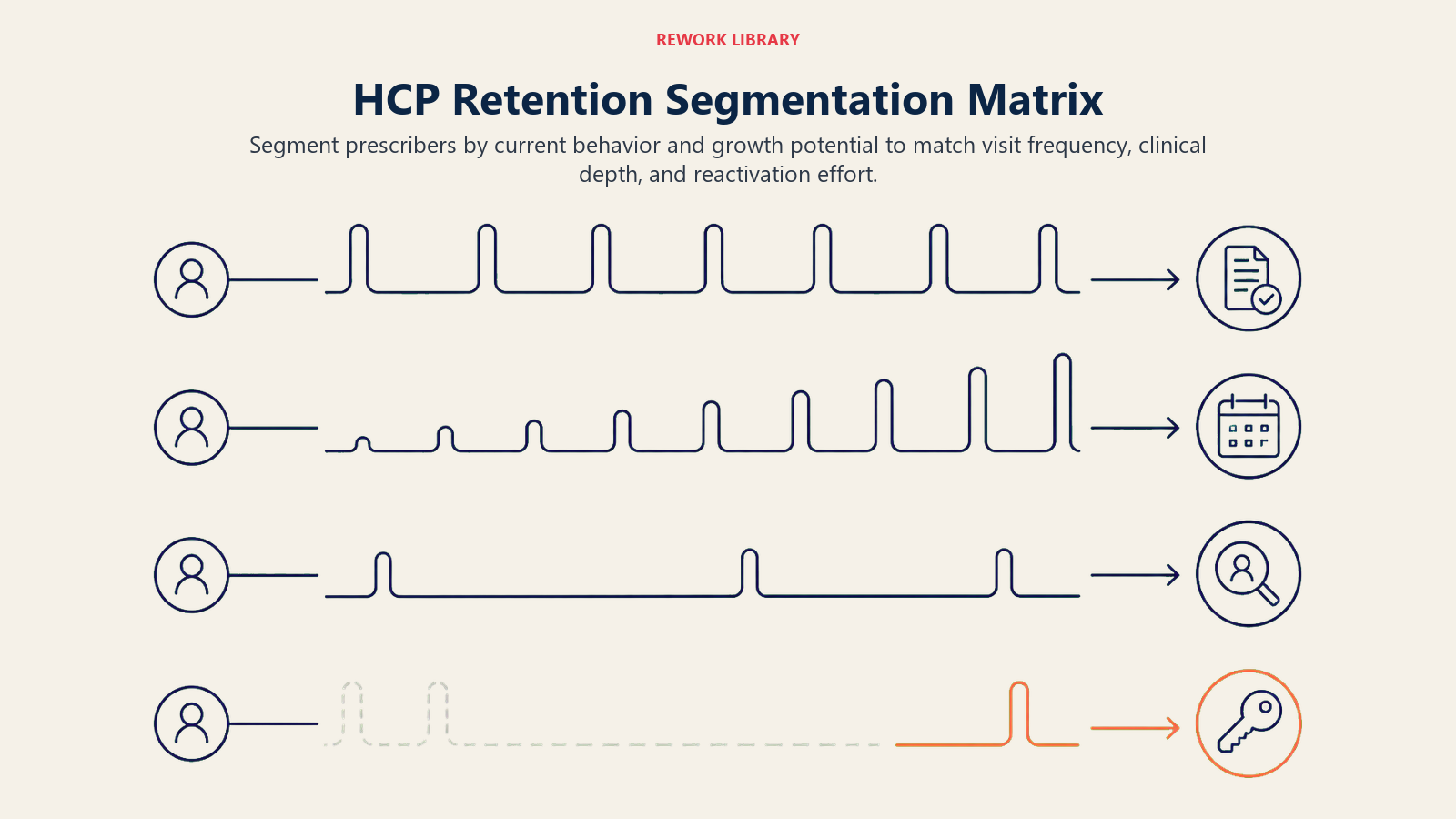
Not every retained prescriber needs the same investment of time, clinical depth, or visit frequency. A segmentation framework that distinguishes between prescribers by current behavior and commercial potential allows the field force to concentrate its highest-value retention efforts where they'll have the most impact. When you rank accounts by both current value and growth potential, you allocate rep time where it compounds rather than spreads effort evenly across accounts with very different ceilings.
HCP Segmentation Matrix
| Segment | Definition | Commercial Behavior | Retention Strategy |
|---|---|---|---|
| High-frequency prescribers | Writing 10+ scripts/month for your brand | Consistent revenue, potential KOL (key opinion leader) candidates | Deepen clinical engagement, peer events, MSL involvement |
| Moderate writers | Writing 3-9 scripts/month, growing trend | Growing but not yet reliable | Increase visit frequency, share outcome data, address prescribing hesitations |
| Occasional prescribers | Writing 1-2 scripts/month, no growth | Trial behavior, not embedded in practice | Identify patient types where they prescribed, replicate conditions |
| Lapsed prescribers | Prescribed previously, no scripts in past 3 months | Lost to competitor or therapeutic change | Reactivation protocol, understand reason for lapse, clinical re-engagement |
The field force effort allocation should follow this segmentation. High-frequency prescribers warrant the most senior engagement, including medical science liaison involvement when clinical questions exceed the rep's scope. Lapsed prescribers require a different kind of conversation entirely: one that acknowledges the absence and seeks to understand what changed, not one that re-runs the standard detail.
Call frequency and coverage optimization provides the quantitative framework for translating this segmentation into territory planning and visit scheduling.
The Retention Visit Agenda
The second, third, and ongoing visits with a retained prescriber should follow a consistent but flexible structure. "Consistent" because having a clear purpose for each visit builds the doctor's expectation that a meeting with your rep is worth their time. "Flexible" because the most valuable conversations are responsive to what the doctor actually brings to the meeting.
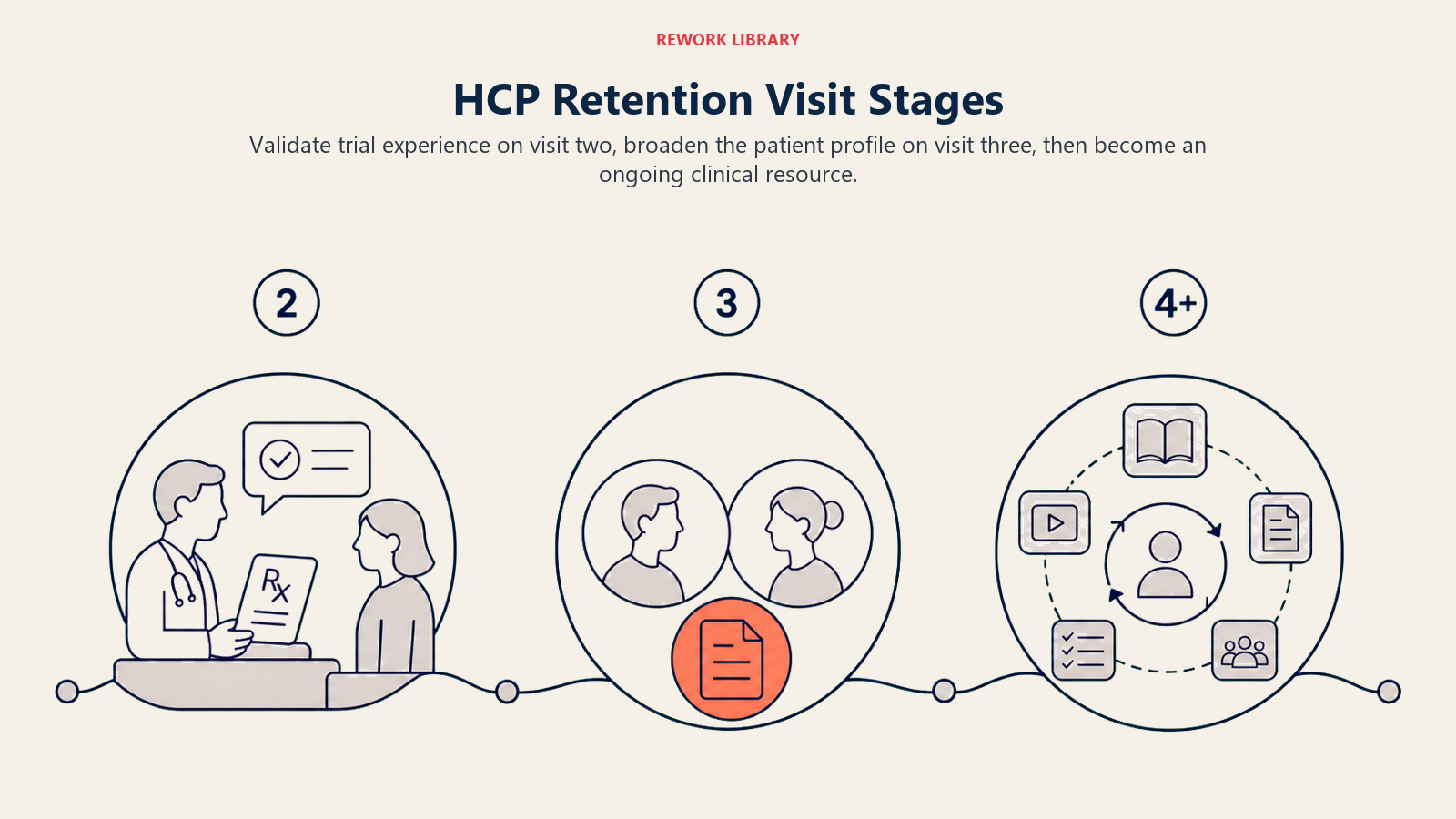 Second Visit: Validating the Trial Experience
Second Visit: Validating the Trial Experience
The second visit is arguably the highest-stakes retention visit. This is where you find out whether the first prescription went well or not. The agenda:
- Ask about the patient they prescribed to. What happened? Was the outcome what they expected?
- If the outcome was positive, help them identify the next appropriate patient profile. Move from "a patient I tried it with" to "patients like this."
- If the outcome raised questions or concerns, address them directly with clinical evidence. Don't minimize or deflect. A doctor who trusts your rep to engage seriously with a clinical concern is more likely to continue prescribing than one who gets a reassuring non-answer.
Third Visit: Broadening the Prescribing Profile
By the third visit, you should understand where the doctor is comfortable prescribing your product and where they're hesitating. The agenda:
- Review any additional patient cases since the last visit
- Introduce data on a patient subgroup adjacent to where they're already prescribing: a second-line versus first-line indication, a comorbidity profile they haven't considered, a patient population they're hesitant about
- Share peer-reviewed evidence or real-world outcome data that addresses their specific hesitations
Ongoing Visits: Clinical Partnership
From the fourth visit onward, the rep's role shifts from product educator to clinical resource. The ongoing visit agenda should include:
- Update on any new clinical evidence, label changes, or indication expansions
- Check-in on patients currently on therapy: any adverse event questions, adherence concerns, or patient feedback the doctor has heard
- Market intelligence the doctor might find valuable: competitor changes, guideline updates, formulary shifts at the hospitals where they practice
- Prompt for patient referrals or peer introductions if the relationship supports it
Clinical Value Delivery
The most effective retention lever available to a medical rep isn't a clinical trial they're carrying in their detailing folder. It's the ability to make the doctor better at managing the patients they're already treating.
Outcome data on their patient population. When you have access to real-world evidence or regional outcome data that reflects the types of patients this doctor treats, share it. Not as a product pitch, but as clinical intelligence. A cardiologist who sees their prescribing pattern reflected in registry data, and who can see that the outcomes match what the clinical trials predicted, gains confidence that extends beyond your product to their clinical judgment.
Patient population insights. If your brand has a broader market, you may have aggregated (and properly anonymized) insights about which patient characteristics predict best response. Sharing that analysis with a prescriber positions your rep as a source of clinical intelligence, not just a salesman with a new slide deck.
Peer-reviewed evidence on emerging questions. Doctors who prescribe a product regularly develop clinical questions that weren't addressed in the original detailing: what happens in patients with this particular comorbidity, what do the three-year outcomes look like, how does this product perform in elderly patients or in patients with renal impairment. A rep who anticipates these questions and arrives with relevant published evidence before the doctor has to ask is delivering genuine clinical value. The PhRMA Code on HCP Interactions sets the industry standard for what constitutes appropriate clinical exchange, drawing a clear line between educational value and promotional activity. Get this balance right and the doctor starts looking forward to the visit.
The patient awareness and adherence programs your company supports can also be shared as clinical value to prescribers. Doctors who know their patients have access to adherence support tools, refill reminders, or patient education resources are more confident prescribing for complex or long-term treatment courses.
How Do You Detect a Competitor Threat Before It Shows in Prescription Data?
The doctors who are most vulnerable to competitor switching are the ones your reps are visiting least frequently. By the time a prescriber has written zero scripts for two consecutive months, the switch has already happened. The commercial response needs to be much earlier.
 Early Warning Checklist: Signs a Prescriber Is Shifting
Early Warning Checklist: Signs a Prescriber Is Shifting
- Shorter visit times on consecutive calls, doctor less engaged or more distracted
- Questions about competitor products or their clinical data
- Mentions of a colleague or KOL who is "having good results" with a competitor
- Reduction in patient referrals they used to make to your brand appropriate cases
- Asking about formulary availability or pricing changes for your product
- Canceling scheduled visits more frequently than before
- Clinical questions about adverse events or tolerability they hadn't raised before
None of these signals alone confirms a shift in progress. But two or more across consecutive visits should trigger a specific retention conversation, not a standard detail. Treating this list as a proactive early-warning checklist is the same principle that applies to any subscription business: the accounts you save are the ones you identified as at-risk before they formally walked away.
The retention conversation when competitive pressure is detected is not a defensive product pitch. It's a clinical inquiry: "I've noticed you've had some questions about [competitor], what's driving that interest?" Understanding the clinical or operational reason for the interest gives the rep something real to address, whether it's a patient experience they misattributed to your product, a formulary change, or a clinical question they haven't had answered.
The prescription-to-pharmacy pull-through alignment tracking system can surface early signals when a prescriber's patterns are diverging from historical volume, before the shift is visible in territory totals.
Escalating to MSLs and KOLs
Some clinical questions and retention challenges exceed the scope of what a medical rep can address. High-value prescribers who have deep clinical expertise, are operating at the boundary of a product's label, or have complex questions about mechanism or long-term data require engagement at a different level.
Medical science liaisons are the appropriate escalation point when:
- The prescriber is asking questions that require a scientific depth beyond the approved label
- There are clinical questions about specific patient populations, dosing scenarios, or adverse events that are outside the rep's scope to address
- The prescriber is a potential speaker, clinical investigator, or KOL candidate who would benefit from peer-level scientific dialogue
Peer-level scientific engagement from MSLs carries particular weight: a pilot study of rare disease prescribers (34 respondents) found that non-promotional personal engagement may be more influential on prescribing decisions than standard promotional rep activity, though the small sample limits generalization beyond the rare disease context studied.
KOL engagement is appropriate when:
- A high-value prescriber is expressing interest in research collaboration, speaker bureau participation, or advisory board input
- A competitor is using peer influence to erode confidence in your brand, and a credible peer advocate is needed to counter that influence
- Peer-to-peer scientific exchange would accelerate the prescriber's adoption of a new indication or patient population
The medical MSL and commercial alignment framework defines the handoff protocol between the field force and the medical affairs team, so escalations happen cleanly and the prescriber receives a seamless experience rather than a fragmented handoff between functions that don't communicate. The question that follows is whether any of this is actually measurable.
Retention KPIs
Managing HCP retention without defined metrics is managing by intuition. The retention disciplines above need to connect to measurable commercial outcomes that tell leaders whether the system is working.
Retention KPI Dashboard (benchmark figures are illustrative targets; calibrate to your therapeutic area and territory baseline)
| KPI | Definition | Measurement Frequency | Illustrative Target Range |
|---|---|---|---|
| Prescriber retention rate | % of active prescribers in period T who are still active in period T+1 | Quarterly | Greater than 80% for top-tier prescribers |
| Average scripts per retained HCP | Total prescriptions across retained HCPs divided by number of retained HCPs | Monthly | Trending upward quarter-on-quarter |
| Lapsed prescriber reactivation rate | % of lapsed prescribers who write at least one script within 90 days of a reactivation visit | Quarterly | Greater than 30% |
| High-frequency prescriber growth | % of moderate writers who move to high-frequency in the following quarter | Semi-annual | Greater than 20% |
| Competitor-threatened account recovery | % of accounts with early-warning signals that maintain volume within 2 quarters of intervention | Quarterly | Greater than 50% |
These KPIs belong in the field force performance dashboard, reviewed in territory-level business reviews and used to evaluate rep retention effectiveness separately from acquisition performance. The two disciplines are different, and measuring them together obscures where the revenue risk actually sits.
The doctor detailing best practices framework connects retention visit quality to these KPIs, giving field leaders a direct line from visit behavior to prescribing outcome.
Retention as the Highest-ROI Use of a Rep's Calendar
The economics of HCP retention favor investment. Acquiring a new prescribing doctor from zero to consistent trial takes multiple visits, clinical evidence delivery, and often months of nurture. Retaining a doctor who is already prescribing requires the same visit cadence but delivers commercial return from the first conversation.
When reps spend their time protecting their existing prescribing base, the territory performs. When they spend it almost entirely on acquisition, chasing new targets while existing prescribers drift, the territory looks active on coverage metrics but bleeds revenue quietly.
The field forces that build durable market positions combine both disciplines with clear allocation rules: minimum visit frequency for retained prescribers by segment, defined retention agendas that differ from acquisition agendas, escalation protocols for competitive threats, and KPIs that hold reps accountable for protecting what they've already built.
That combination, systematic acquisition plus systematic retention, is what converts field force investment into compounding commercial return.
The HCP Segmentation Retention Matrix is the core framework this article describes: four prescriber segments defined by current behavior and growth potential (high-frequency writers, moderate writers, occasional prescribers, and lapsed prescribers), each with a distinct commercial behavior profile and a distinct retention strategy. High-frequency prescribers get deepened clinical engagement and MSL involvement. Moderate writers get increased visit frequency and outcome data. Occasional prescribers need the specific patient conditions that prompted their trial replicated in new patient identification. Lapsed prescribers require a reactivation protocol that diagnoses the reason for the gap before attempting to rebuild prescribing confidence.
The matrix drives field force time allocation in a way that a uniform visit schedule cannot. When a rep applies the same visit type and frequency to all four segments, they over-invest in accounts where less would maintain the relationship and under-invest in accounts at risk of full lapse. Segment-based allocation concentrates the highest-value retention effort where it will have the most commercial impact.
Learn More

Senior Implementation Consultant
On this page
- HCP Retention vs HCP Acquisition: Different Disciplines
- Segmenting Retained HCPs
- The Retention Visit Agenda
- Clinical Value Delivery
- How Do You Detect a Competitor Threat Before It Shows in Prescription Data?
- Escalating to MSLs and KOLs
- Retention KPIs
- Retention as the Highest-ROI Use of a Rep's Calendar
- Learn More