Marketing and Field Sales Alignment in Pharma: Turning Brand Strategy into Territory Execution
 Here's a scene that plays out in pharma companies every year, usually about six weeks after the annual brand plan is finalized.
The brand marketing team has spent three months developing a well-crafted campaign: a sharp positioning statement, a clinically differentiated message, beautifully produced detail aids, patient support materials, and a conference presence timed to the major medical meeting in the therapy area. The investment is real: the brand plan represents months of cross-functional input and millions in promotional spend.
Here's a scene that plays out in pharma companies every year, usually about six weeks after the annual brand plan is finalized.
The brand marketing team has spent three months developing a well-crafted campaign: a sharp positioning statement, a clinically differentiated message, beautifully produced detail aids, patient support materials, and a conference presence timed to the major medical meeting in the therapy area. The investment is real: the brand plan represents months of cross-functional input and millions in promotional spend.
Turn this article into takeaways for your work.
Each assistant summarizes the article only for you and suggests best practices for your work.
Then the field force goes to work. The reps take the detail aids, put them in their bags, and within two weeks most of them have reverted to their own version of the product story. The doctor they visit most often doesn't want to see the branded visual, so they skip it. The approved messaging doesn't land well in their territory's patient population, so they adapt it. The campaign runs. The reps make their calls. But the message the health care professionals (HCPs) receive bears little resemblance to what the brand team created.
That's the strategy-execution gap. And in pharma, it costs companies not just promotional effectiveness but regulatory exposure and HCP trust.
Why Pharma Marketing and Field Sales Drift Apart
The drift isn't random. It's structural, driven by three differences that rarely get resolved at the organizational level.
Key Facts: The Marketing-Field Misalignment Tax

- A commonly cited commercial excellence observation holds that a substantial share of pharma promotional materials printed and distributed to field forces are never used in a customer call, wasting both production cost and the MLR review investment behind each piece. The precise figure varies by study and company; the pattern itself is widely recognized across pharma commercial organizations.
- The FDA's warning letters to pharmaceutical companies document enforcement actions stemming from off-label promotional violations, many of which originate when reps deviate from approved messaging without structured brand-field alignment in place (FDA: https://www.fda.gov/drugs/enforcement-activities-fda/warning-letters-and-notice-violation-letters-pharmaceutical-companies).
- The PhRMA Code on Interactions with Health Care Professionals identifies every rep-HCP interaction as a professional touchpoint that should benefit patient care, reinforcing why inconsistent field messaging creates both commercial and compliance risk.
Different incentives. Brand managers are measured on brand equity metrics, message recall scores, market research outputs, and promotional material utilization. Medical reps are measured on call frequency, prescriber coverage, and territory prescription volume. These metrics don't connect. A brand manager who produces an award-winning detail aid is not measured on whether reps use it. A rep who consistently hits their script targets is not penalized for deviating from the approved message. The incentive systems pull in different directions.
Different timelines. Marketing works on annual brand plans, campaign cycles, and pre-launch sequences that run 12-18 months ahead. Field sales lives in weekly call plans, monthly target reviews, and quarterly performance cycles. A brand campaign launched in Q1 is already being re-evaluated by the marketing team in Q2 while field managers are still coaching reps on basic call structure. The planning horizons don't align.
Different definitions of success. Marketing sees success at the brand level: awareness, positioning strength, share of voice, net promoter scores among target HCPs. Field sales sees success at the territory level: scripts written, prescribers covered, high-decile HCPs moved to prescriber status. These are related outcomes but they're rarely measured in an integrated way that shows the contribution of each team to the other's success.
The result is what commercial excellence professionals call the misalignment tax: budget spent on promotional materials that don't reach HCPs, campaigns that generate awareness but not prescription change, and field messaging that creates compliance risk because it wasn't reviewed against the approved label. The OIG compliance program guidance for pharmaceutical manufacturers identifies promotional practices as one of the principal risk areas regulators scrutinize.
The Misalignment Tax: What It Costs You
The misalignment between marketing and field sales creates concrete costs that show up in commercial performance.
Promotional materials that go unused. Across pharma commercial organizations, a substantial share of printed and distributed promotional materials never reach an HCP in a structured call. Detail aids designed by marketing, reviewed by the medical-legal-regulatory (MLR) team, and shipped to representatives sit in bags and car trunks while reps tell the product story in their own words. The production cost is wasted. The MLR review investment is wasted. And the HCP is getting an uncontrolled version of your brand message.
Off-label promotion risk. When reps deviate significantly from the approved promotional messaging, they can inadvertently make claims that aren't supported by the label, reference data from studies not approved for promotional use, or respond to unsolicited questions in ways that cross the promotional boundary. The compliance risk isn't hypothetical: the FDA's warning letters to pharmaceutical companies document enforcement actions that result from promotional violations, and off-label exposure remains among the most significant legal risks in the industry. Marketing-field misalignment is a root cause.
Inconsistent HCP experience across territories. Your cardiologist in one city is getting a different message about your product than your cardiologist in another. In a therapy area where HCP peer influence drives prescribing norms, inconsistent messaging creates inconsistent advocacy. The word-of-mouth that spreads at medical conferences reflects whatever message individual reps chose to use, not the brand strategy.
Wasted media and congress investment. When marketing runs a conference presence at a major medical meeting and follows it up with a detailing push, the campaign only delivers its full value if reps are carrying the same message that the congress symposium communicated. If reps haven't been briefed, trained, and equipped to reinforce the conference message, the campaign investment is disconnected from the territory execution that converts awareness into prescribing decisions.
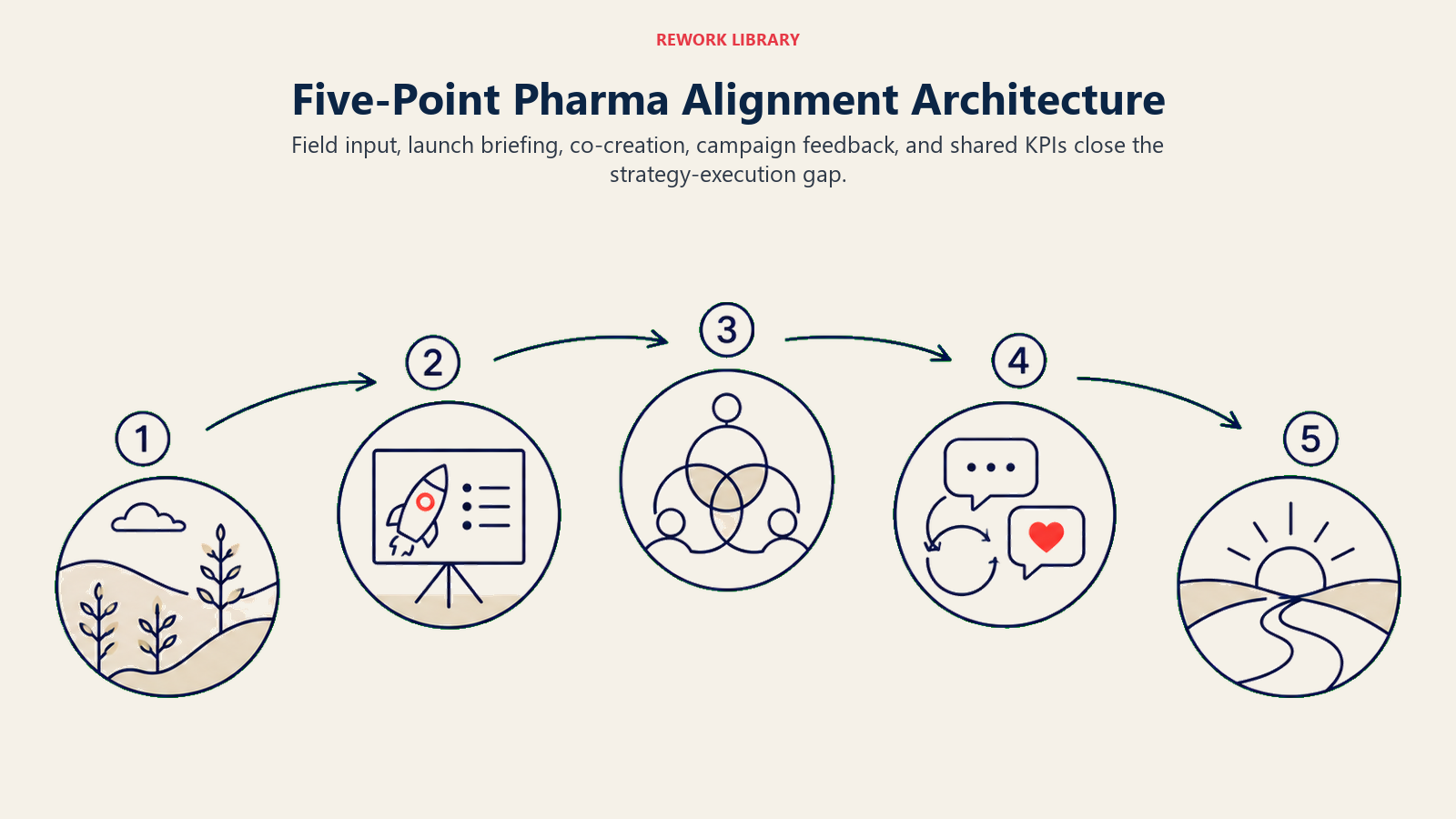
What Are the Five Integration Points That Close the Strategy-Execution Gap?
Closing the strategy-execution gap requires structured integration at five points across the product lifecycle and commercial calendar. These aren't one-time fixes. They're recurring operational mechanisms. The Five-Point Alignment Architecture names this structure: Brand Plan Field Input, Pre-Launch Strategy Briefing, Detail Aid Co-Creation, Campaign Feedback Loop, and Shared KPIs. Each integration point addresses one of the three structural misalignments (incentives, timelines, and definitions of success) that cause marketing and field to drift.
Integration Point 1: Brand Plan Input from the Field
The brand plan should not be built in a marketing conference room and handed to the field. It should be built with field intelligence that comes from the territory.
Before the annual brand planning cycle concludes, brand managers need structured input from field managers and senior medical representatives on: which clinical messages resonate with prescribers in practice, what objections HCPs raise most consistently in calls, which patient types the prescribers see most and what motivates their therapeutic choices, and what competitors are saying in the territory that brand messaging needs to address.
This input doesn't replace the market research that the brand team commissions. It grounds it. HCPs answering a market research survey and HCPs responding to a rep in a consulting room are often giving different signals. Both matter. Only one of them currently gets into most brand plans.
Integration Point 2: Pre-Launch Strategy Briefing (Not Product Training)
Field training programs for product launches are usually strong on clinical knowledge and weak on brand strategy. Reps leave launch training knowing the mechanism of action, the efficacy data, the safety profile, and the approved indication. They often leave without understanding the positioning logic: why this product, for this patient, communicated this way, at this moment in the competitive landscape.
The pre-launch briefing that closes this gap is not another training module. It's a brand strategy session led by the brand manager directly, answering the questions that motivate field execution: What problem are we solving for this prescriber? Why should this doctor change their behavior? What's the specific patient type where we win? What does success look like for their patients and for their practice?
When reps understand the "why" behind the brand strategy, they adapt the message for their territory in ways that are consistent with the strategy rather than departures from it. When they only know the "what" of the product features, they go off-script because the script doesn't feel real to them.
Integration Point 3: Detail Aid Co-Creation with Field Testing
Detail aids developed entirely in marketing without field testing almost always fail in practice. The visual that looks impressive on a conference room screen doesn't work when a rep is sitting across from a doctor who has four minutes between patients and no interest in a product monograph.
Co-creation means taking visual aid concepts to field testing with a representative sample of reps and HCPs before finalization. The questions to answer: Does this message land in a 90-second conversation? Does this visual make the clinical point without explanation? Is there a slide the rep would never use because it creates an objection instead of addressing one?
Field-tested detail aids have higher utilization rates because reps were part of building them. This isn't a minor benefit. A detail aid used in 80% of target HCP calls delivers four times the value of one used in 20%.
Integration Point 4: Campaign Feedback Loop from Call Reports
Field reporting and closed-loop marketing is the mechanism by which the territory speaks back to the brand team. When reps complete call reports that capture not just activities (calls made, samples dropped) but content signals (which messages the HCP responded to, what objections were raised, what competitor mentions appeared), that data becomes brand intelligence.
Most pharma CRM systems collect call reports. Most marketing teams don't read them. Closing this loop requires two things: a call report template that captures strategically useful information rather than just compliance checkboxes, and a monthly brand review process that includes analysis of call report content trends as a standard input.
The feedback loop isn't just about validating that messages are being delivered. It's about learning which messages are working with which prescriber segments so the brand team can refine, adjust, and optimize the campaign in-cycle rather than waiting for the annual brand plan revision.
Integration Point 5: Shared KPIs That Connect Brand to Territory
The most powerful structural change in marketing-field alignment is replacing parallel KPI systems with shared metrics that make the connection explicit.
| Siloed Metric | Shared Replacement |
|---|---|
| Marketing: detail aid recall score | Shared: message recall by territory (combines marketing data with rep call report output) |
| Field: call frequency on target HCPs | Shared: target HCP prescribing conversion rate (connects call activity to Rx outcome) |
| Marketing: campaign reach (impressions, congress attendees) | Shared: new prescriber acquisition by territory post-campaign |
| Field: territory script volume | Shared: script lift vs. baseline, by territory, attributed to campaign exposure |
Shared KPIs don't emerge naturally. They require a decision at the commercial leadership level: marketing effectiveness will be measured at the prescribing point, not at the campaign production level. That shift in measurement philosophy changes where people focus their energy. It mirrors the logic behind RevOps metrics in B2B commercial organizations, where the same problem of siloed marketing and sales metrics applies: when both functions share a single set of revenue-connected numbers, the internal negotiation about whose work matters stops and the focus shifts to the outcome that actually counts. Pharma commercial leaders facing the same siloed-metrics problem will recognize the pattern.
See the Prescription Demand Generation article in the Learn More section for how these shared metrics connect to territory-level prescribing outcomes.
Closed-Loop Marketing in Practice
Closed-loop marketing in pharma means that every promotional activity, whether a detail aid call, a digital touchpoint, a congress symposium, or a patient support referral, generates data that flows back to the brand team and informs the next wave of promotional investment.
The data flow works like this:
Field call report data captures which messages were used in which HCP conversations, what objections arose, and whether the HCP showed prescribing intent signals. This flows into the CRM.
CRM analytics aggregate call report data by message, by HCP segment, by territory, and by time period. The brand team can see message utilization rates and objection frequency patterns.
Prescription audit data (IQVIA, IMS, or equivalent) shows whether call activity in a territory is correlating with prescribing change. Territories where call activity is high but prescribing isn't moving have a message problem, a targeting problem, or a HCP relationship problem, each requiring a different intervention.
Brand team optimization uses these inputs to refine messaging, retarget promotional investment, update detail aids in-cycle, and brief field managers on territory-level adjustments for the next campaign period.
This loop doesn't work without discipline. It requires that call reports actually contain useful content data, that someone in the brand team is accountable for synthesizing field intelligence monthly, and that the findings actually change something about the promotional plan rather than just informing a PowerPoint slide.
The detail aid and visual aid toolkit that reps carry is the most visible artifact of the marketing-field relationship. The Detail Aid and Visual Aid Usage article in Learn More covers how field-tested materials change utilization rates.
Governance Model: Brand-Field Alignment Committee
The five integration points described above don't sustain themselves through goodwill. They need a governance structure with clear ownership, a defined cadence, and an escalation path when alignment breaks down. Brand-Field Alignment Committee: Recommended Structure
| Meeting | Frequency | Participants | Agenda |
|---|---|---|---|
| Campaign alignment briefing | At launch of each major campaign | Brand manager, field manager(s), medical affairs rep, MLR representative | Campaign strategy review; field team Q&A; approved message confirmation |
| Monthly performance review | Monthly | Brand manager, commercial excellence, field manager | KPI bridge review; call report trend analysis; material utilization rates |
| Quarterly brand-field strategy session | Quarterly | Brand director, field director, commercial excellence director | Strategy vs. execution audit; upcoming campaign preview; field intelligence synthesis |
| Annual brand plan field input session | Annual (Q3 for following year plan) | Brand manager, brand director, senior field reps, field managers | Territory intelligence input; prescriber segment feedback; competitive intelligence from the field |
The escalation path matters. When there's a sustained disconnect between brand strategy and field execution, the commercial director needs to own the resolution. That might mean investing in better field training, simplifying the detail aid, adjusting the brand message for the realities of the territory, or making a difficult decision about which campaign elements to de-prioritize.
Marketing effectiveness is not measured in the boardroom. It's measured at the moment a rep is sitting across from a prescriber and the message either lands or it doesn't. Governance exists to make sure someone is accountable for that moment.
For the downstream impact on prescriptions reaching patients, see prescription-to-pharmacy pull-through alignment.
HCP Relationship as the Measurement Point
The fundamental principle of marketing-field alignment in pharma is that brand strategy only creates value when it reaches the HCP through a representative who understands and believes it. A brand plan that lives in a PowerPoint presentation is not strategy. It's an aspiration. The strategy becomes real in the room with the doctor, when the rep translates positioning into a conversation that connects clinical evidence to patient need in a way that motivates prescribing change.

That translation requires the rep to be not just trained on the product but aligned with the brand strategy. It requires doctor detailing best practices that embed the brand message into the call structure. It requires feedback loops that tell the brand team whether the message is working. And it requires shared accountability so that marketing and field succeed or fail together, measured by the same prescribing outcomes.
Companies that get this right don't just run better campaigns. They build HCP relationships where the brand message is consistent, the clinical positioning is credible, and the representative is seen as a genuine source of relevant medical information rather than a rotating door of promotional visitors. The PhRMA Code on Interactions with Health Care Professionals sets the industry standard for how those relationships should be conducted, reinforcing that every touchpoint between a rep and a prescriber should benefit patient care rather than simply advancing a promotional objective.
That's what brand strategy looks like when it actually works.
Frequently Asked Questions about Marketing and Field Sales Alignment in Pharma
What is the marketing-field misalignment tax in pharma?
The misalignment tax is the aggregate commercial cost of brand strategy that fails to execute in territory. It includes the cost of unused detail aids, the compliance exposure from off-label promotional deviation, inconsistent HCP messaging across territories, and the disconnection between congress or media investment and field follow-through. Across pharma commercial organizations, a significant share of printed promotional materials never reach an HCP in a structured call, a pattern widely recognized even where precise numbers are not published.
Why do pharma brand managers and medical reps use different success metrics?
Brand managers are measured on brand equity metrics, message recall scores, and promotional material utilization. Reps are measured on call frequency, prescriber coverage, and territory prescription volume. These metrics don't connect: a brand manager is not assessed on whether reps use the detail aid, and a rep is not penalized for deviating from approved messaging. The incentive gap is structural, not attitudinal, which is why fixing it requires shared KPIs, not better communication.
What is closed-loop marketing in pharma?
Closed-loop marketing means that every promotional activity generates data that flows back to the brand team and informs the next wave of investment. Field call reports capture which messages HCPs responded to and what objections arose. CRM analytics aggregate those signals by message, segment, and territory. Prescription audit data shows whether call activity is correlating with prescribing change. The brand team uses these inputs to refine messaging and retarget investment in-cycle rather than waiting for the annual brand plan revision.
How do you co-create a detail aid with field input?
Take visual aid concepts to testing with a representative sample of reps and HCPs before finalization. The key questions are whether the message lands in a 90-second conversation, whether the visual makes the clinical point without explanation, and whether any slide creates an objection rather than resolving one. Field-tested materials have higher utilization because reps participated in building them and believe in the message.
What shared KPIs connect marketing effectiveness to field outcomes?
Instead of marketing measuring detail aid recall and the field measuring call frequency separately, shared replacements include message recall by territory that combines marketing data with call report output, target HCP prescribing conversion rate that connects call activity to Rx outcomes, new prescriber acquisition by territory attributed to campaign exposure, and script lift versus baseline by territory. These metrics create joint accountability for the prescribing outcome rather than parallel accountability for upstream activities.
What is the governance structure for brand-field alignment?
An effective alignment committee runs four meetings: a campaign alignment briefing at each major campaign launch, a monthly performance review covering KPI bridges and call report trends, a quarterly brand-field strategy session for strategy-execution audits, and an annual brand plan field input session in Q3. The escalation path when sustained disconnect appears runs to the commercial director, who owns the resolution.
Learn More

Senior Implementation Consultant
On this page
- Why Pharma Marketing and Field Sales Drift Apart
- The Misalignment Tax: What It Costs You
- What Are the Five Integration Points That Close the Strategy-Execution Gap?
- Integration Point 1: Brand Plan Input from the Field
- Integration Point 2: Pre-Launch Strategy Briefing (Not Product Training)
- Integration Point 3: Detail Aid Co-Creation with Field Testing
- Integration Point 4: Campaign Feedback Loop from Call Reports
- Integration Point 5: Shared KPIs That Connect Brand to Territory
- Closed-Loop Marketing in Practice
- Governance Model: Brand-Field Alignment Committee
- HCP Relationship as the Measurement Point
- Learn More