Market Access KAM and Field Sales Alignment: Translating Formulary Wins into Territory Revenue
Turn this article into takeaways for your work.
Each assistant summarizes the article only for you and suggests best practices for your work.
Market access secures a national formulary listing after 18 months of dossier work, payer negotiations, and pricing concessions. The field force doesn't hear about it until a rep stumbles across a mention in a payer newsletter. Meanwhile, the next three months of prescription data show no uptick in the newly reimbursed molecule.
This is one of the most expensive alignment failures in pharma commercial operations. Not because the access team did poor work, and not because the field force isn't working hard. But because the organizational handoff from access win to territory activation never happened. The listing exists on paper and nowhere else.
Market access opens the door. Field alignment determines whether anyone walks through it. These two functions are not sequential: they need to be coordinated throughout the product lifecycle for an access win to produce the revenue it was negotiated to deliver.
What Market Access and KAM Actually Do
Before building the alignment model, it's worth being precise about what each function owns and where their work ends.
Market access teams negotiate with payers: national and regional health insurance bodies, government formulary committees, managed care organizations, and regulatory bodies that govern reimbursement. Their deliverables are formulary listings (getting the product on the approved drug list), reimbursement dossiers (the clinical and health-economic evidence package), pricing agreements (the price at which the payer reimburses), and access restriction management (navigating step therapy, prior authorization, and prescriber restrictions that limit who can prescribe and under what conditions).
A formulary win is a commercial achievement. But it doesn't automatically generate prescriptions. It creates the legal and reimbursement context within which prescriptions can be written and filled. Payers use tiering, rebate negotiations, and competitive positioning to shape formulary access by therapeutic area, which means the access architecture varies significantly by drug class. The gap between "can be prescribed" and "is being prescribed" is where field alignment matters.
KAM (Key Account Management) teams operate at the institutional level: major hospital systems, health networks, specialized clinics, and institutional tenders. They negotiate hospital formulary listings (getting the product onto the hospital's approved drug list), secure tender contracts (winning volume-based supply agreements), and manage long-term relationships with pharmacy committees, medical directors, and procurement. In many markets, especially for specialist products, KAM determines whether the product exists inside the institution at all.
But a KAM win at the hospital formulary level doesn't mean that individual oncologists, neurologists, or department heads are prescribing. That habit formation happens at the ward level, during rep calls, in peer conversations, and through clinical champions. KAM opens the institutional door; the field rep builds the prescribing behavior inside.
Key Facts: Market Access and Field Alignment
- Deloitte analysis of US drug launches from 2012 to 2021 found that 57% of launch underperformance was attributed to limited market access capabilities, not clinical shortcomings (Deloitte, "Rethinking Market Access," 2022).
- A 2024 cross-sectional study across 561 insurance formularies found roughly 40% of antiemetic medications prescribed for cancer patients face at least one utilization management restriction such as prior authorization or step therapy, illustrating the access barriers that field teams must navigate in oncology and supportive care (PMC12501812).
- Payers use tiering, rebate negotiations, and competitive positioning to shape formulary access by therapeutic area, meaning the access architecture the field must navigate varies significantly by drug class (Deloitte, pharmaceutical pricing and market access).
The Translation Problem: From National Win to Territory Script
There's a structural reason this handoff fails. Market access and KAM teams operate at the national, regional, or institutional level. Their metrics are formulary coverage rate, access restrictions negotiated away, and contracts won. Field teams operate at the territory and HCP level. Their metrics are calls made, prescriptions written, and market share by outlet.
These two operating realities rarely share a direct communication channel, which creates three predictable translation failures. The Access-to-Script Activation Model names this challenge directly: it describes the four structured handoffs (field input into negotiation, listing briefing, objection translation, and segment refresh) that convert a national access win into territory-level prescribing behavior. Without all four handoffs operating, the access investment produces formulary coverage but not scripts.
Formulary listing doesn't reach HCP awareness. An HCP in a territory prescribing a competitor's product doesn't know your product is now reimbursed at a preferred tier unless someone tells them. A formulary announcement goes to the payer's member communications and perhaps a formulary database. It doesn't go to the prescriber's inbox. The rep is the delivery mechanism. But if the rep hasn't been briefed on the listing, its scope, and its patient eligibility criteria, they can't deliver the message accurately or confidently.
Hospital listing doesn't translate to ward-level prescribing. A KAM win secures the hospital formulary. That listing means the product is available in the pharmacy and can be dispensed. It doesn't mean the cardiologists in ward 4 know it's listed, don't know the reimbursement pathway for their specific patient population, or have changed their prescribing habits. The KAM team's job ends at institutional approval. Habit formation inside the institution is field work. See the institutional sales framework in Hospital and Institutional Tender Sales.
Access restrictions confuse reps in the field. Step therapy requirements mean a prescriber must try and fail another drug before your product can be prescribed. Prior authorization means the prescriber needs to submit supporting documentation before the payer covers the script. These restrictions are pervasive: a 2024 cross-sectional study across 561 formularies found roughly 40% of antiemetic medications for cancer patients faced at least one utilization management restriction, including prior authorization and step therapy requirements. In therapeutic areas beyond oncology the specific rates vary, but coverage friction is a consistent pattern reps must be ready to navigate. When reps encounter objections about prior auth or step therapy, they often can't explain the pathway clearly, because no one briefed them on the specific access architecture of the market access team's deal. The HCP's perception: complicated, not worth the hassle. Four structured handoffs prevent every one of these failures.
The Alignment Model: Four Handoff Moments
Sustainable alignment between market access, KAM, and field sales doesn't come from a single launch meeting. It requires structured handoffs at four distinct points in the product lifecycle.
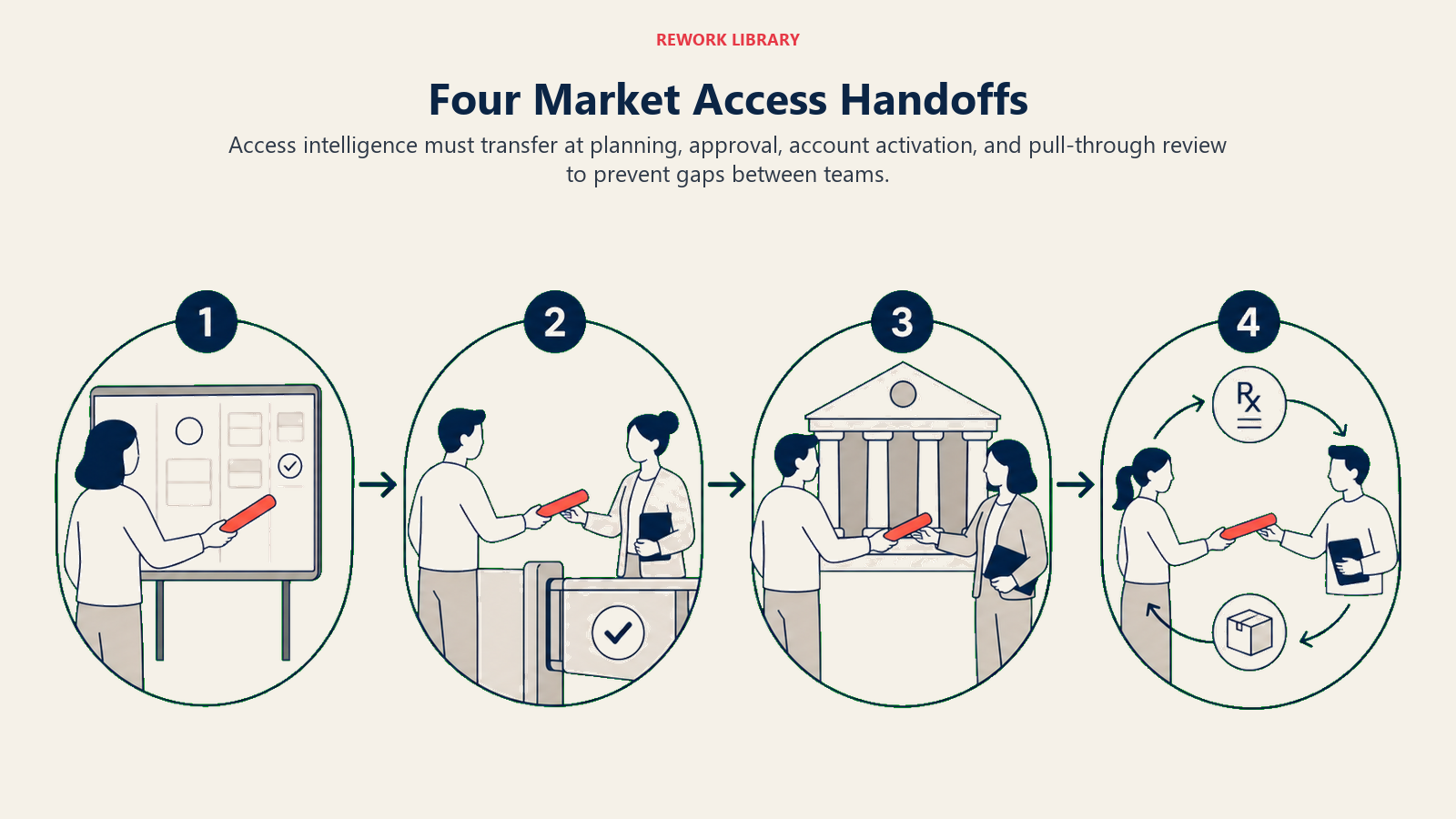
Handoff 1: Pre-Launch, Field Input into Negotiation Strategy
Before the access team finalizes its negotiation position with a payer, the field has information they don't. Territory managers know which access barriers HCPs complain about most. They know whether step therapy is a deal-breaker for prescribers in their region or a manageable administrative step. They know which restrictions will effectively block uptake and which won't matter.
This input shapes the negotiation. If the access team knows that prior authorization takes 4 days on average in a key region and that prescribers routinely abandon the process, they can negotiate harder to remove it. If they know that the competitor's preferred tier status is the primary objection in field calls, they prioritize tier position over list price.
Field input at this stage is commercially valuable to the access team and relatively low-burden to collect: a structured pre-negotiation survey of 10-15 territory managers, or a dedicated session in the regional sales meeting, produces the insight without major process overhead. This is also the moment to apply a rigorous patient-profile filter: the Opportunity Qualification criteria that commercial teams use to assess deal potential translate naturally here into defining which prescriber segments represent realistic adoption candidates given the access restrictions being negotiated, which payer types, which therapeutic areas, and which patient eligibility thresholds will determine true prescribing potential.
Handoff 2: Listing Announcement, Field Activation Briefing
When a formulary listing is confirmed, the access team needs to produce a field activation brief. This isn't the dossier. It's a one-page (or one-slide) summary that tells the field what they need to know to convert the listing into prescriptions.
| Element | What the Field Needs |
|---|---|
| Formulary tier and position | What tier is the product on? What's the patient co-pay? |
| Eligible patient population | Which patients qualify under this listing? |
| Prescriber restrictions | Any HCP specialty restrictions or approval requirements? |
| Access restrictions | Is there step therapy? Prior authorization? What are the steps? |
| Timing and geography | Which regions or payers? Effective date? |
| HCP-ready talking points | How to communicate the access win in a 2-minute call |
Without this brief, the field will either not use the listing at all or use it incorrectly, which erodes prescriber trust when the claim doesn't match reality at the pharmacy.
Handoff 3: Objection Translation, Payer Language to Rep Response
Payer objections are stated in payer language. Step therapy requirements, formulary exceptions, prior authorization criteria, non-preferred tier status: these are the terms in which access restrictions are documented. But HCPs and pharmacists don't speak in these terms when they object. They say "this is too much paperwork," "my patients can't afford the co-pay," or "I've tried getting this approved before and it never goes through."
The access team understands both the payer language and the underlying commercial reality. The field rep hears the objection and often doesn't know how to bridge them. An objection translation guide resolves this.
| Payer Restriction | HCP Objection Form | Rep Response |
|---|---|---|
| Step therapy (must fail Drug A first) | "My patients have to try the old drug first, which delays treatment" | "Yes, and most patients complete the step in under 3 weeks. Here's a step therapy support form that takes 10 minutes." |
| Prior authorization required | "The prior auth process takes forever and my office won't do it" | "We have a PA support service that handles the paperwork. Your office submits one form and we manage the rest." |
| Non-preferred tier (higher co-pay) | "My patients can't afford this, it's too expensive" | "For patients on [payer name], we have a co-pay assistance card that brings cost to $X. Here's the enrollment link." |
| Specialty prescriber restriction | "I can't prescribe this, only specialists can" | "Correct for the general formulary. But you can submit a formulary exception for patients who meet [criteria X]. Here's the exception form." |
Building this guide is access team work. Distributing and training on it is a field leadership responsibility. See the pre-call planning context in Pre-Call Planning and Objection Handling.
Handoff 4: Segment Refresh, Ongoing Access Updates
Formulary status changes. Tier positions shift during annual plan negotiations. New restrictions get added or existing ones removed. A payer win in one region doesn't carry to another. And in markets with multiple payer channels, the access picture at the territory level is complex and constantly moving.
Most pharma companies send quarterly formulary updates to the field in a spreadsheet. Most reps don't read it. The fix is not more data: it's targeted alerts by territory. If payer X changes your product's tier in a region, the territory managers covering that region need a push notification, not a buried column in a multi-tab spreadsheet.
This requires sales ops to build the territory-to-payer mapping that allows market access updates to be filtered and targeted. It's a systems and process investment, but it's what makes the ongoing segment refresh actually land in the field. See the targeting principles in Customer Segmentation and Targeting.
KAM-Field Coordination in Institutional Accounts
Hospital accounts require a distinct coordination model because the decision-making structure is layered. KAM secures the formulary listing. But inside the institution, prescribing behavior is driven by individual physicians, department heads, and pharmacists who may or may not know the product is listed.
A KAM-field coordination model for institutional accounts typically works like this:
KAM owns the formulary and the institutional relationship. Their contacts are pharmacy directors, medical committee members, and procurement. They're managing the listing and any volume-based agreements.
Field reps own HCP relationships inside the institution. They're calling on cardiologists, endocrinologists, or whichever specialty is relevant. Their job after a KAM win is to inform and engage the prescribers, explain the formulary status, and support first prescriptions.
Joint planning happens before the KAM win and within 2 weeks after. Before the listing, KAM briefs the field on which institutions are in negotiation and which clinical champions have been identified (physicians who participated in clinical trials or have advocacy relationships). After the listing, KAM and field map the institution together: which departments, which HCPs, which sequence of calls. The layered stakeholder structure inside a hospital account is a genuine multi-stakeholder challenge: pharmacy committees, medical directors, and ward-level prescribers are distinct decision nodes, each with different priorities and different access to the formulary decision. The Multi-Stakeholder Navigation framework maps this kind of parallel influence structure, useful prep for KAM teams planning a hospital account entry after a formulary win.
Shared metrics track conversion. A KAM win is the leading indicator. Prescription data from inside the institution is the lagging outcome. Tracking both in a shared dashboard tells you whether the access win is translating into prescribing behavior. This connects directly to the demand generation work described in Prescription Demand Generation.
Shared Metrics: Measuring the Access-to-Prescription Chain
Most pharma commercial dashboards track access metrics (coverage rate, formulary listings) and field metrics (calls, market share) in separate reports. Alignment requires a shared view that connects the two.
| Metric | Definition | Owned By |
|---|---|---|
| Formulary access coverage rate | Percentage of target HCPs covered by a formulary listing (any tier) | Market access |
| Preferred access coverage rate | Percentage of target HCPs covered by a preferred-tier listing | Market access |
| Unreimbursed prescription rate | Percentage of prescriptions written that are not covered (proxies access gaps) | Sales ops + market access |
| Formulary utilization rate | Percentage of prescriptions written in covered markets vs. potential | Field + market access |
| Access barrier conversion rate | Percentage of HCPs who raised access objections and subsequently prescribed | Field |
| KAM account activation rate | Percentage of KAM-listed hospital accounts with at least 1 prescription in the quarter | KAM + field |
The formulary utilization rate is the most important joint metric. It asks: of all the prescriptions that could be written in markets where we have access, what percentage actually are? A high access coverage rate with a low formulary utilization rate means the access team's work isn't reaching the prescriber. That's an alignment failure, and it's measured and actionable. Most commercial leaders have never seen both numbers on the same dashboard. The next section is about what happens when they finally do.
High coverage with low utilization is the fingerprint of a failed activation handoff: the access work landed, but nobody briefed the field to convert it.
Access Without Activation Is Wasted Negotiation
It costs significant commercial resources to secure a formulary listing: medical affairs investment, health economics work, pricing negotiations, and often pricing concessions that affect the brand's P&L for years. That investment only generates a return when field-level activation converts the listing into prescriptions.
The alignment model described here isn't complex. Four structured handoff moments, a shared metrics dashboard, an objection translation guide, and a KAM-field coordination protocol for institutional accounts. None of these require a major organizational restructure. They require commercial leadership to own the handoff process explicitly rather than assuming it happens organically.
Field without access wastes every call on a product the HCP can't prescribe for covered patients. Access without field activation wastes every negotiation on a listing that produces no prescriptions. The two functions are co-owners of the revenue event. Build the operating model that treats them that way.
Frequently Asked Questions about Market Access KAM and Field Sales Alignment
What is the difference between market access and field sales in pharma?
Market access negotiates with payers and formulary bodies to secure the reimbursement and tier position that allow a product to be prescribed for covered patients. Field sales engages prescribers directly to build the clinical confidence and prescribing habit that converts that coverage into actual scripts. Access determines what the field can sell; the field determines how much of that potential gets realized.
Why do formulary wins often fail to translate into prescription growth?
Three failure modes account for most of the gap. First, HCPs in the territory never learn the product is reimbursed because no field briefing occurred. Second, reps are not prepared to explain access restrictions like step therapy or prior authorization, so prescribers default to the path of least resistance. Third, KAM hospital wins don't trigger ward-level engagement, so individual physicians inside the institution remain unaware of the formulary listing.
What should a field activation brief contain after a formulary win?
A functional brief covers six elements: the formulary tier and patient co-pay, the eligible patient population, any prescriber specialty restrictions, the specific access restrictions and how to navigate them, the geographic and payer scope with effective date, and HCP-ready talking points the rep can deliver in a two-minute call. Anything longer than one page is likely to be ignored.
How should KAMs and field reps coordinate inside hospital accounts?
KAM owns the institutional relationship: pharmacy committee, medical director, and procurement. The field rep owns HCP relationships inside the institution: the cardiologists, endocrinologists, or relevant specialists. Joint planning happens before the KAM win (to identify clinical champions) and within two weeks after (to map which departments and HCPs need engagement and in what sequence). Shared metrics track whether the listing is producing prescriptions.
What is the formulary utilization rate and why does it matter?
Formulary utilization rate measures what percentage of prescriptions that could be written in covered markets actually are written. A high access coverage rate combined with a low utilization rate is the signature of an alignment failure: the access work landed but the field activation did not. Tracking this metric jointly forces market access and field leadership to own the gap together.
How often should market access update the field on formulary changes?
Quarterly updates are the minimum standard, but they should be delivered as targeted territory alerts rather than multi-tab spreadsheets. If payer X changes your product's tier in a specific region, only the territory managers in that region need immediate notification. Untargeted updates produce low engagement. Targeted alerts produce action.
Learn More

Senior Implementation Consultant
On this page
- What Market Access and KAM Actually Do
- The Translation Problem: From National Win to Territory Script
- The Alignment Model: Four Handoff Moments
- Handoff 1: Pre-Launch, Field Input into Negotiation Strategy
- Handoff 2: Listing Announcement, Field Activation Briefing
- Handoff 3: Objection Translation, Payer Language to Rep Response
- Handoff 4: Segment Refresh, Ongoing Access Updates
- KAM-Field Coordination in Institutional Accounts
- Shared Metrics: Measuring the Access-to-Prescription Chain
- Access Without Activation Is Wasted Negotiation
- Learn More