Hospital and Institutional Tender Sales: Winning Formulary Listings and Tender Contracts That Drive Volume

Turn this article into takeaways for your work.
Each assistant summarizes the article only for you and suggests best practices for your work.
A physician prescribes your product. The patient takes the prescription to the hospital pharmacy. The pharmacist checks the formulary. Your product isn't listed. The patient gets something else, something that is listed, and the prescription your medical rep spent months generating drives volume for a competitor.
This scenario plays out every day in markets where institutional access hasn't been secured. The doctor's prescription is a necessary condition for institutional sales. It isn't a sufficient one. Getting from prescription to dispensed product inside a hospital requires a separate sales track: formulary listing, tender award, or direct institutional agreement, each with its own stakeholders, timeline, and decision logic.
Commercial leaders who treat hospital selling as a scaled-up version of retail pharmacy selling consistently underperform in institutional channels. The skills overlap only partially. The stakeholders, timelines, and commercial dynamics of institutional sales are fundamentally different, and they require a dedicated approach.
How Institutional Buying Works
Retail pharmacy selling is a relatively direct relationship: the rep calls on the pharmacist, who makes or influences stocking decisions, and sell-out follows from patient demand and pharmacist recommendation.
Institutional buying is a committee process mediated by budget controls, clinical standards, and procurement regulations. The decision to add a product to a hospital formulary or to award a tender is rarely made by any single person. It requires alignment across clinical, pharmacy, procurement, and finance functions, often over a timeline measured in months.
Three mechanisms govern institutional product access:
Formulary listing: The hospital formulary is the approved drug list used by clinical staff. A product not on the formulary cannot be dispensed by the hospital pharmacy, regardless of individual prescriber preference. Formulary listing decisions are made by a Formulary Committee (sometimes called a Pharmacy and Therapeutics Committee, or P&T Committee) on a defined review schedule, typically quarterly or semi-annually.
Tender contract: Government hospitals and large private hospital groups often procure pharmaceuticals through a formal tender process. Suppliers submit bids against defined specifications. The contract is awarded based on clinical criteria, price, and supplier capability. Tender contracts typically run one to three years and can cover substantial volume.
Direct institutional agreement: Some private hospitals and hospital groups negotiate direct purchasing agreements outside formal tender processes. These involve commercial negotiation with a procurement team and typically require key account engagement at the organization level.
Understanding which mechanism applies to each institution in the territory is the first step in institutional account planning.
Key Facts: Hospital and Institutional Tender Sales
- Research on pharmaceutical tender design in expanding health systems shows that lowest-price-only awards increase the risk of drug shortages and supplier market exits, reinforcing why commercial teams must model downstream channel impact before submitting a tender price.
- Total timeline from tender notice to first order is typically 6 to 18 months, with contract award alone taking 2 to 6 weeks post-evaluation; actual duration varies by market, institution size, and procurement framework.
- WHO prequalification of medicines sets internationally recognized supplier eligibility criteria that national procurement agencies commonly mirror in tender specifications, meaning pre-qualification documentation must be maintained in an always-ready state, not assembled after a tender notice appears.
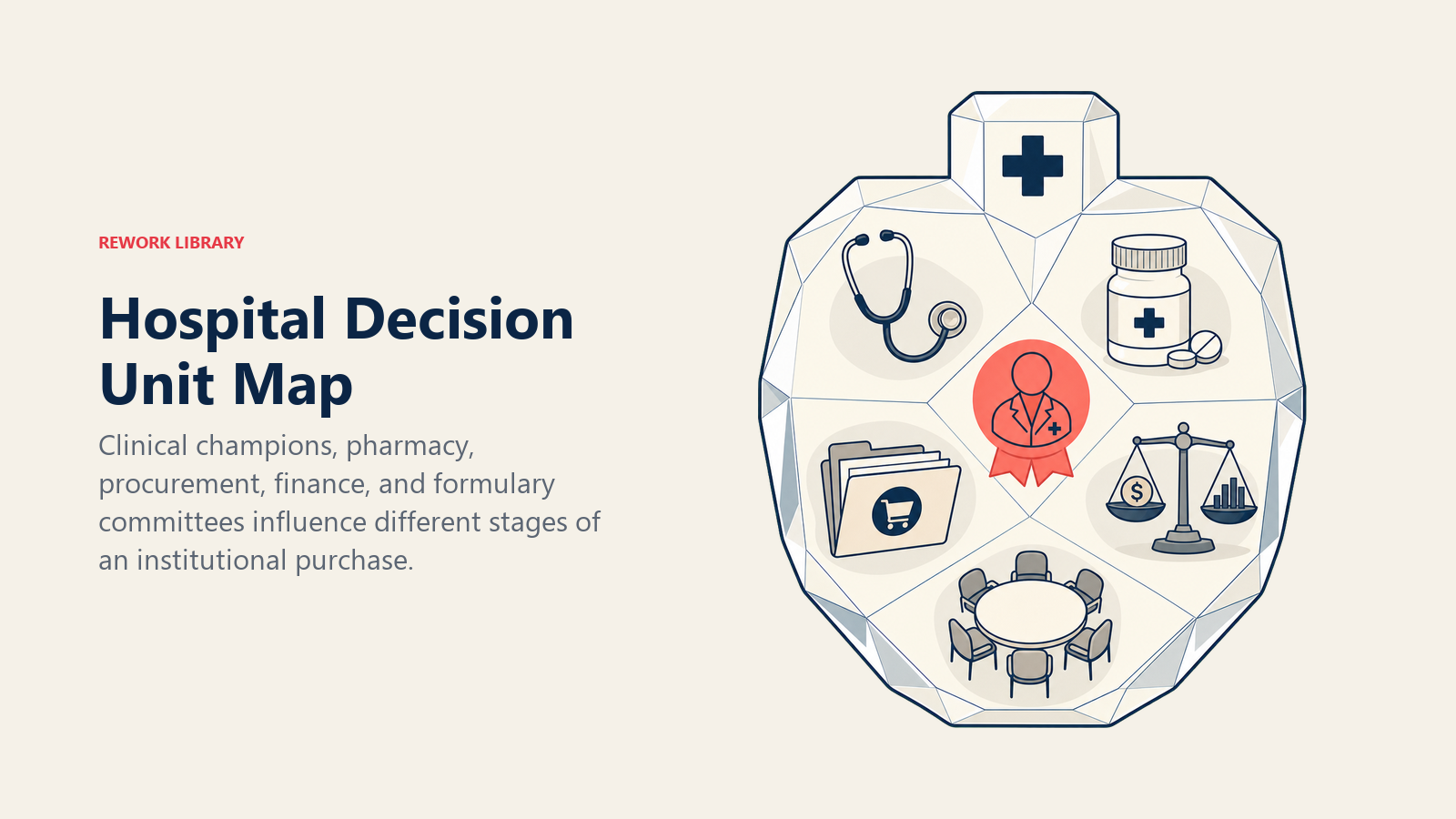
Mapping the Hospital Decision Unit
The hospital's decision unit for pharmaceutical procurement is not a single buyer. It's a network of stakeholders with different interests, different levels of authority, and different timelines for engagement. Getting a formulary listing or tender award requires managing all of them. The same discipline that governs multi-stakeholder navigation in complex B2B deals applies here: identify who holds influence at each stage, map their individual concerns, and engage them in the right sequence rather than pitching the same message to everyone at once.
Clinical Lead (Prescribing Champion)
The clinical lead is the physician, department head, or specialist who has the therapeutic expertise and credibility to advocate for a product inside the institution. Without a clinical champion, a formulary submission is a document with no internal advocate. With one, it's a clinical recommendation backed by a respected colleague.
The clinical champion's role is to present the clinical case for listing, to respond to committee questions about evidence, and to communicate urgency when treatment options are inadequate. Finding and developing this champion is often the first and most important task in institutional account development. See KOL (key opinion leader) identification and recruitment for the framework.
Pharmacy Director (Formulary Gate)
The pharmacy director controls formulary submission logistics and often chairs or co-chairs the Formulary Committee. They set the submission requirements, the review schedule, and the technical criteria for evaluation. They're also the practical administrator of the formulary: they know which products are under pressure from budget constraints, which therapeutic categories have competing listings under review, and where the committee's clinical priorities lie.
Building a working relationship with the pharmacy director before a submission is critical. A cold submission from an unknown rep lands in a queue. A submission that the pharmacy director has been briefed on, that they understand the clinical rationale for, and that has been prepared to their technical standards, moves faster and encounters fewer administrative obstacles.
Procurement Officer (Price and Contract)
The procurement officer manages the commercial evaluation: price per unit, volume commitments, payment terms, and compliance with tender specifications. In government hospitals, this role may sit within a central government procurement agency rather than the hospital itself.
Procurement officers are not clinical decision-makers. Their primary concern is defensible value for money within regulatory requirements. The commercial submission must speak their language: per-unit cost, total contract value, pricing stability, and delivery performance track record.
Finance Director (Budget Holder)
The finance director's concern is the net budget impact of adding a new product. This is not simply the product's price: it's the net cost versus current alternatives, adjusted for dosing frequency, treatment duration, and any downstream cost offsets (reduced hospitalization days, fewer complications, shorter treatment course).
A health-economic argument that shows a higher-priced product reducing total treatment cost is more persuasive to the finance director than a clinical argument about mechanism of action. The commercial team needs to translate clinical superiority into budget impact language.
Medical Superintendent or CMO (Final Sign-Off)
In many institutional settings, the medical superintendent or chief medical officer holds final approval authority for new formulary additions or significant tender changes. They're rarely involved in the detailed review process, but they sign off on the outcome. Their priorities are institutional reputation, clinical governance risk, and strategic alignment with the hospital's therapeutic focus areas.
Hospital Decision Unit Map:
| Stakeholder | Primary Concern | Engagement Timing | Rep vs. KAM vs. Medical Affairs |
|---|---|---|---|
| Clinical Champion | Clinical evidence, patient outcomes | Early and continuous | Medical Affairs / MSL (Medical Science Liaison) |
| Pharmacy Director | Formulary integrity, submission quality | Pre-submission to post-listing | KAM (key account manager) |
| Procurement Officer | Price, compliance, vendor capability | Commercial evaluation phase | KAM / Commercial team |
| Finance Director | Budget impact, cost-effectiveness | During evaluation, especially for premium-priced products | KAM with health-economics support |
| Medical Superintendent / CMO | Institutional reputation, governance | Final approval stage | Senior KAM / Medical director |
The Tender Process Step by Step
Tender processes vary by market and institution, but the underlying structure is consistent. Understanding the sequence allows a commercial team to prepare at each stage rather than scrambling to catch up.
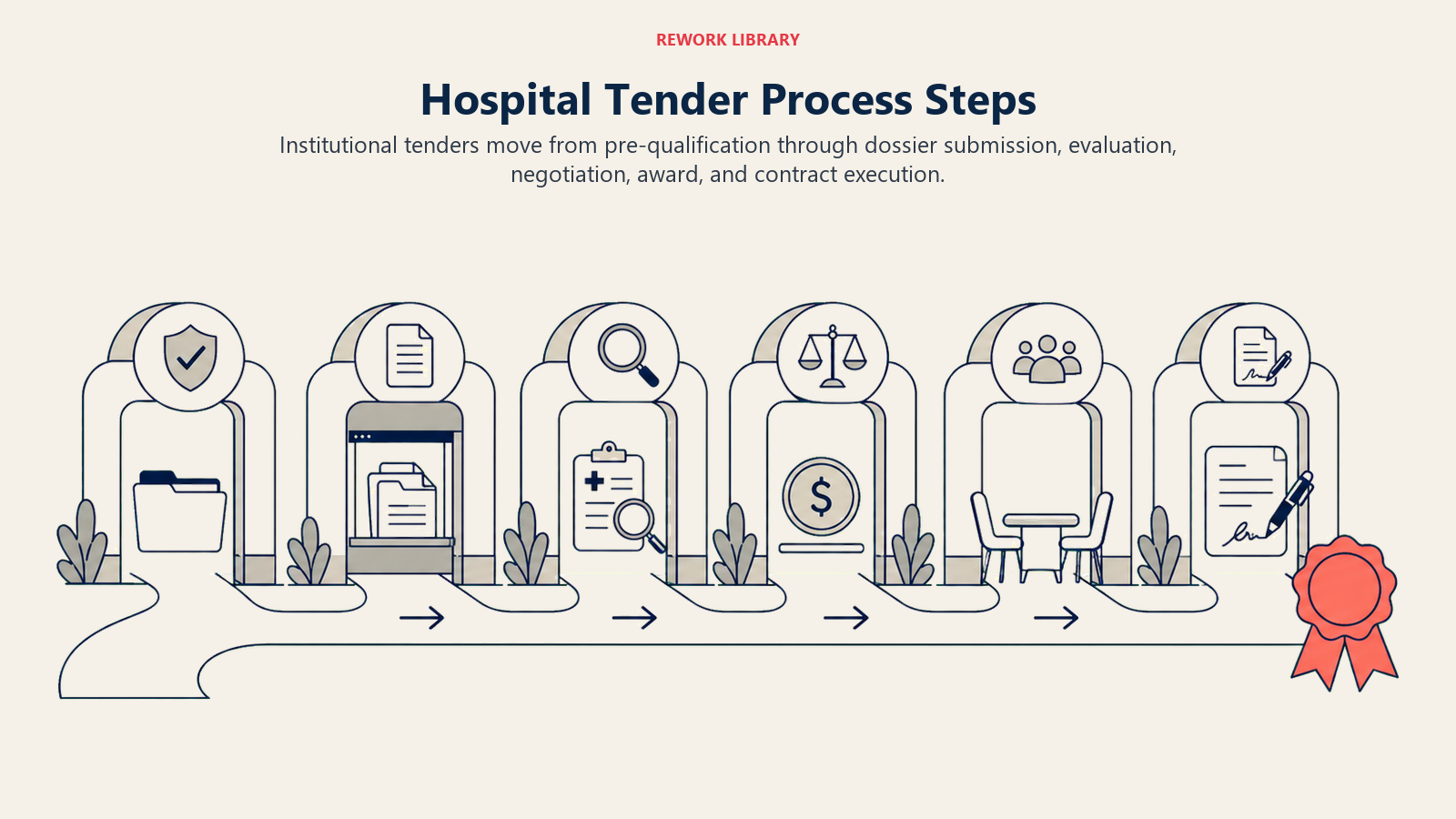
Stage 1: Expression of Interest and Pre-Qualification
Many formal tender processes require suppliers to register interest and demonstrate basic eligibility: regulatory approval, manufacturing standards, distribution capability, and financial stability. Pre-qualification documentation should be maintained in an always-ready state, not assembled after a tender notice appears. A supplier who misses the pre-qualification window is excluded from the entire tender cycle. WHO prequalification of medicines sets out internationally recognized supplier eligibility criteria that national procurement agencies commonly mirror in their own tender specifications.
Stage 2: Technical Evaluation (Clinical Data Submission)
The technical envelope contains the clinical dossier: efficacy data from clinical trials, safety profile, comparative effectiveness against current standard of care, and (increasingly) pharmacoeconomic data. The evaluating committee scores technical submissions against defined criteria.
The clinical dossier must be prepared to regulatory standards, but it must also be readable by committee members who are clinicians, not regulatory specialists. The executive summary and the head-to-head comparison tables are the parts that get read under time pressure. They need to be clear, concise, and directly responsive to the institution's stated clinical priorities.
Stage 3: Commercial Evaluation (Price, Terms, Volume Commitment)
The commercial envelope is evaluated separately from the technical submission in most formal processes, to prevent price from influencing clinical assessment. The commercial evaluation covers price per unit, pricing for different pack sizes and presentations, volume commitments from the institution and counter-commitments from the supplier, payment terms, and service level requirements (delivery frequency, cold chain capability, emergency supply protocols).
Pricing strategy for institutional tender is distinct from retail pricing. Institutional tender prices are typically lower than retail and can create reference pricing risk if not managed carefully. Research on pharmaceutical tender design in expanding health systems shows that lowest-price-only awards increase the risk of drug shortages and supplier market exits, reinforcing why the commercial team must assess the downstream impact of tender pricing on retail and parallel trade channels before submitting a price.
Stage 4: Award and Contract Execution
The tender award is communicated to all bidders. The winning supplier enters contract negotiation with the procurement office, finalizing terms, volume schedules, and service commitments. Contract execution includes regulatory documentation, supply agreements, and (in government contracts) formal gazetting of the award.
Contract execution is not the start of revenue. It's the start of the relationship that will determine whether formulary listing translates into actual volume.
Tender Process Timeline (Indicative):
| Stage | Typical Duration | Key Action |
|---|---|---|
| Pre-qualification | 2 to 4 weeks | Submit standard dossier, confirm eligibility |
| Technical preparation | 4 to 12 weeks | Clinical dossier, health-economic model |
| Technical evaluation | 4 to 8 weeks | Committee review, clarification responses |
| Commercial evaluation | 2 to 4 weeks | Price negotiation, terms alignment |
| Award and contracting | 2 to 6 weeks | Legal review, contract execution |
| First order | 2 to 8 weeks post-award | Pull-through activation begins |
Total timeline from tender notice to first order is typically 6 to 18 months depending on market and institution, with significant variation across procurement frameworks. Commercial teams that treat tender award as the revenue event consistently underperform against teams that begin pull-through preparation during the commercial evaluation stage. Understanding the expected duration of each stage is the institutional equivalent of tracking sales cycle length: when you know how long each phase takes on average, you can forecast revenue more accurately and allocate KAM resources before the crunch hits.
Formulary Listing Strategy
A formulary submission without internal advocacy rarely succeeds on the clinical evidence alone, regardless of how strong the evidence is. The formulary strategy combines clinical dossier quality with stakeholder preparation.

Clinical Dossier Preparation
The core of the dossier is comparative clinical evidence: your product versus the current standard of care, presented in the format the committee expects. This typically includes:
- Regulatory approval status and indication wording
- Efficacy data (primary endpoints from pivotal trials)
- Safety profile (adverse event rates versus comparator)
- Dosing and administration requirements
- Head-to-head or indirect comparison data where available
- Post-marketing safety data if the product has been on market
Medical Affairs and MSL alignment is essential at this stage. The clinical team prepares and defends the dossier. The commercial team ensures the submission reaches the right committee at the right time with the right internal champion in place.
Health-Economic Argument
Budget-constrained formulary committees increasingly require a cost-effectiveness argument alongside clinical evidence. The health-economic model should address:
- Cost per treatment course versus current standard
- Downstream cost offsets (avoided hospitalizations, reduced complications)
- Budget impact analysis (total spend change if the product achieves X% market share within the institution)
- Patient outcome model (quality-adjusted life years, if relevant to the therapeutic area)
This is not territory for the field rep to prepare independently. It requires the commercial support of a health-economics specialist or medical affairs team. But the KAM needs to understand the model well enough to explain the headline numbers to the pharmacy director and finance director in plain language.
When to Bring in MSL Support
MSL (Medical Science Liaison) engagement at key institutions before a formulary submission significantly improves outcomes. The MSL builds clinical credibility separately from the commercial relationship, prepares the clinical champion to present effectively to the committee, and responds to questions about data interpretation that a commercial KAM isn't equipped to address.
The MSL-commercial coordination model requires clear handoff protocols. The KAM owns the commercial relationship and tracks the account plan. The MSL owns the scientific relationship and the clinical champion development. Both need to be aligned on timing, messaging, and the account's specific clinical priorities. A strong dossier with no internal champion is still a long shot.
Pricing Dynamics in Institutional Sales
Institutional pricing is one of the more complex commercial decisions in pharmaceutical sales, and one of the most consequential for markets with reference pricing frameworks.
Tender Price vs. Retail Price
Institutional tender prices are almost always lower than retail pharmacy prices, reflecting volume, contractual certainty, and competitive pressure in the bidding process. The pricing gap between institutional and retail channels is commercially manageable if controlled. It becomes a problem when:
- Institutional prices are published or discoverable, creating external reference prices that pull down retail pricing
- Parallel traders move product from low-price institutional channels to retail markets
- Payers or regulators use institutional tender prices as the basis for reimbursement rates in retail settings
Managing this risk requires commercial teams to understand the reference pricing framework in their market before submitting a tender price. Some markets allow institutional and retail prices to be treated as separate categories. Others apply institutional tender prices as a ceiling on all channel pricing.
Volume Commitments
Tender contracts often include volume commitments from both sides: the institution commits to minimum purchase volumes, and the supplier commits to supply reliability and price stability. Volume commitments are worth negotiating. An institution that commits to volume gives the supplier demand certainty. A supplier commitment to supply reliability protects the institution from shortages and justifies giving the supplier a price concession.
Avoid open-ended volume commitments without a floor. Tender contracts where the institution agrees to "use the product as needed" with no minimum volume guarantee give the supplier no revenue certainty and provide minimal commercial value beyond the formulary listing itself. And a formulary listing without revenue is just a permission slip.
Why Is There a Gap Between Formulary Listing and First Order?
Formulary listing is an access milestone, not a revenue event. Between the listing decision and the first dispensed prescription, several barriers commonly delay or reduce institutional volume.
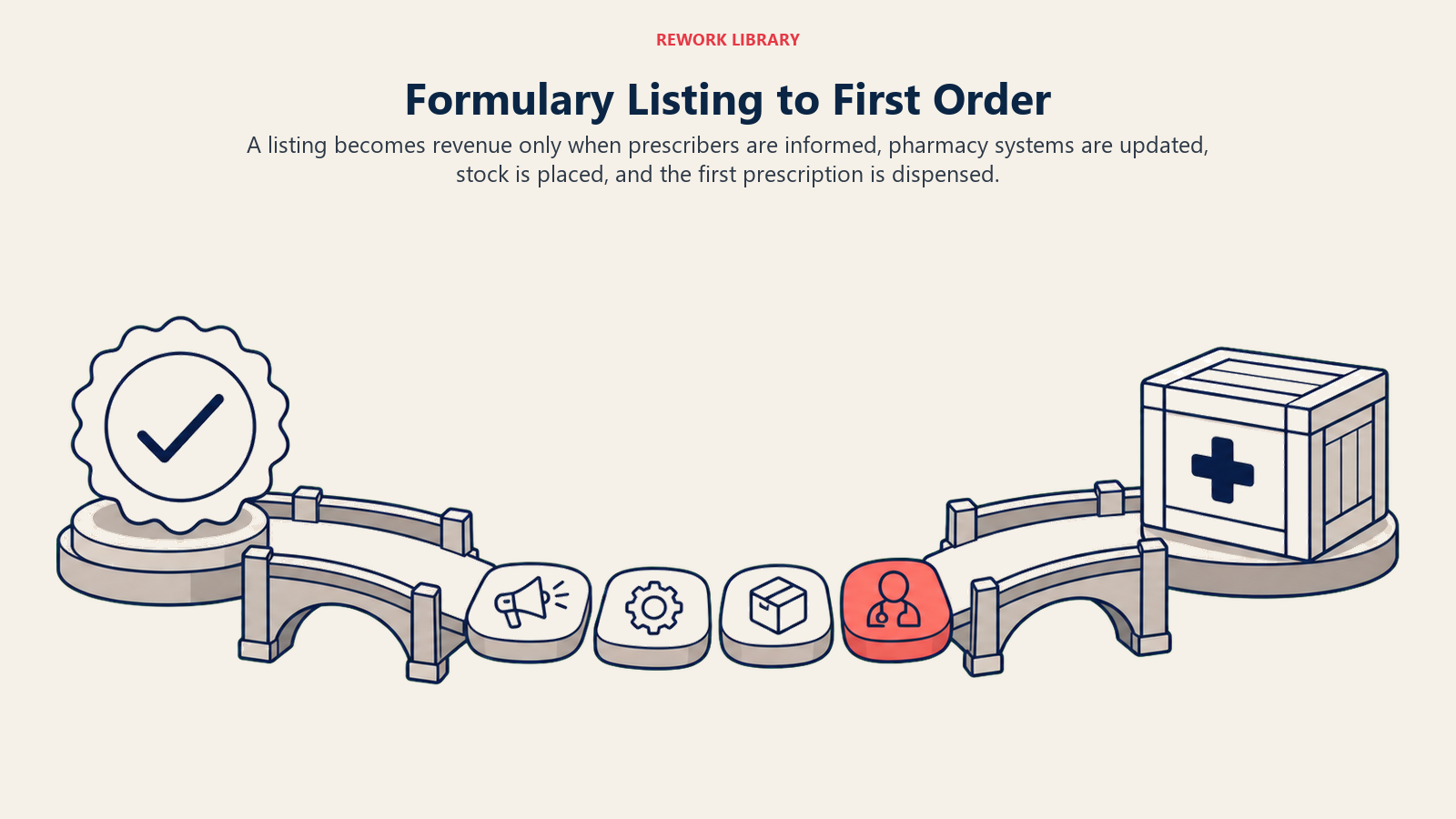
The Listing-to-First-Order Gap
The formulary committee approves a listing. The pharmacy director updates the formulary database. The clinical staff are notified, perhaps via a brief email announcement. Three months later, the product hasn't been ordered once because prescribers weren't aware the listing had been granted, or weren't prompted to change their prescribing habits.
This gap is common and preventable. It requires active pull-through management starting from the moment the listing is confirmed.
Pull-Through Actions After Formulary Win:
| Action | Owner | Timing | Purpose |
|---|---|---|---|
| Clinical champion announcement | MSL / KAM | Within 1 week of listing | Use champion's credibility to notify peers |
| Pharmacist briefing | KAM | Within 1 week | Ensure pharmacy team knows how to dispense |
| Prescriber communications | Medical Affairs | Within 2 weeks | Letters, case presentations, grand rounds slots |
| Sample / starter pack availability | Field rep | Within 2 weeks | Enable trial for new prescribers |
| Initial stock order confirmation | KAM + field rep | Week 2 to 4 | Confirm adequate initial inventory |
| First-use data review | KAM | 30 to 60 days post-listing | Identify prescribers not yet using, address barriers |
Prescription-to-pharmacy pull-through alignment applies inside the institutional setting as much as it does in retail. A prescription written on a ward that doesn't translate to a dispensed product is a data failure and a commercial failure.
The market access and KAM field sales alignment framework determines who owns each pull-through action. Market access secures the listing. Field sales drives prescriber uptake and monitors early dispensing data. The KAM coordinates between functions and tracks account-level performance against the targets in the account plan. But pull-through is only half the institutional game: the other half is protecting what you've already won.
Relationship Management Between Tender Cycles
A tender cycle might last one to three years. The gap between tender award and the next tender opening is not a period to go quiet. It's the period when the relationship equity that determines the next tender outcome is built or eroded.
Between tender cycles, institutional relationship management has three objectives:
Maintain clinical champion commitment: Clinical champions change roles, retire, or face institutional pressures that shift their advocacy priorities. Ongoing MSL engagement keeps the relationship current and identifies changes in the champion's situation early enough to adapt. See HCP relationship retention for the detailed framework.
Build evidence in the institution: Post-marketing data from the institution's own patient population is the strongest input for the next formulary review. Work with the clinical team to capture outcomes data, patient satisfaction measures, and any cost-offset evidence that can be used in the renewal submission. An institution that has been tracking positive outcomes is a strong internal advocate for contract renewal.
Monitor competitive activity: Competitors don't stop working during your contract period. They're building relationships, submitting new clinical data, and preparing for the next tender. The KAM who only re-engages at tender opening is consistently disadvantaged against a competitor who has been active throughout the contract period.
Relationship maintenance activities between tender cycles:
- Quarterly review meetings with pharmacy director to discuss supply performance and utilization trends
- Annual clinical data update with the prescribing champion (new publications, real-world evidence)
- Educational event participation (department grand rounds, clinical conference support)
- Supply performance reviews with procurement (on-time delivery, shortage incidents, complaint handling)
These activities have no direct commercial outcome in the short term. They determine who wins the next tender.
Frequently Asked Questions about Hospital and Institutional Tender Sales
What is a formulary committee and how does it affect pharma sales?
A formulary committee, often called a Pharmacy and Therapeutics (P&T) Committee, is the body that decides which drugs a hospital is permitted to dispense. A product not on the formulary cannot be issued by the hospital pharmacy regardless of individual prescriber preference. These committees review submissions on a defined schedule, typically quarterly or semi-annually, and evaluate clinical evidence, safety data, cost-effectiveness, and alignment with institutional therapeutic priorities. A commercial team that files a submission without understanding the committee's schedule or clinical focus will wait for the next review cycle, often adding three to six months to an already long timeline.
How long does a hospital tender process typically take?
From tender notice to first order, a typical range is 6 to 18 months, though actual duration varies significantly by market, institution size, and procurement framework. As a planning guide: pre-qualification takes 2 to 4 weeks; technical preparation and clinical dossier development takes 4 to 12 weeks; technical evaluation runs 4 to 8 weeks; commercial evaluation adds 2 to 4 weeks; award and contracting adds 2 to 6 weeks; first order follows 2 to 8 weeks post-award. Commercial teams that forecast institutional revenue against a shorter timeline consistently miss their projections. Build a conservative window into account plans and resource allocation for every tender in the pipeline.
What is the listing-to-first-order gap and how do you close it?
The listing-to-first-order gap is the period between a formulary committee approving a product and that product being ordered and dispensed. It is common and preventable. It happens because prescribers are not automatically notified of new formulary additions, pharmacists may not know how to order a new product, and clinical habits take time to change. Closing the gap requires an active pull-through plan deployed the week the listing is confirmed: clinical champion announcement, pharmacist briefing, prescriber communications from medical affairs, initial stock order confirmation, and a first-use data review at 30 to 60 days post-listing.
How should institutional pricing be handled to avoid reference pricing risk?
Institutional tender prices are almost always lower than retail prices, reflecting volume and competitive bidding. The risk is that those lower prices become reference points that pull down retail pricing elsewhere in the market, or that payers use tender prices as a ceiling for reimbursement. Before submitting an institutional price, commercial teams must understand whether their market treats institutional and retail pricing as separate categories or whether a filed tender price becomes public and discoverable. Some markets allow full channel separation; others do not. This is a market access decision, not a sales decision, and it should involve regulatory and commercial leadership before any number appears in a tender submission.
What should a KAM do between tender cycles to protect the renewal?
The relationship work that determines renewal happens during the current contract, not at the next tender opening. Between cycles: run quarterly reviews with the pharmacy director on supply performance and utilization trends; support annual clinical data updates with the prescribing champion; participate in department grand rounds and clinical conference support; and conduct supply performance reviews with procurement. Competitors are building relationships during your contract period. The KAM who goes quiet after award and re-engages only when the new tender opens is consistently disadvantaged in renewals against a competitor who has been active throughout.
When should MSLs be involved in institutional accounts?
Medical Science Liaisons should be involved before a formulary submission, not after. MSL engagement builds scientific credibility with the clinical champion separately from the commercial relationship, prepares the champion to present effectively to the committee, and addresses clinical questions that a commercial KAM is not equipped to handle. The MSL-commercial handoff requires clear protocols: the KAM owns the commercial relationship and account plan; the MSL owns scientific engagement and clinical champion development. Both need to be aligned on timing and messaging so the institution receives a consistent, coordinated experience from both functions.
The Five-Stakeholder Hospital Decision Unit is the institutional account model this article describes: Clinical Lead (prescribing champion), Pharmacy Director (formulary gate), Procurement Officer (price and contract), Finance Director (budget impact), and Medical Superintendent (final sign-off). Each stakeholder has a distinct primary concern and a distinct engagement timing, meaning no single message or single rep can cover the account. The commercial team allocates responsibility by role: Medical Affairs or MSL handles the clinical champion; the KAM handles pharmacy and procurement; senior KAM with health-economics support handles finance; and the medical director or senior commercial leader handles the final sign-off relationship.
Managing this unit correctly requires knowing which stakeholder to engage at which stage, rather than pitching the same clinical evidence deck to everyone. A finance director who hears mechanism-of-action data is being given the wrong conversation. A clinical champion who gets per-unit cost comparisons before clinical evidence review will shut down. Sequence and audience matching are the disciplines that convert a strong dossier into an actual listing.
Conclusion: Winning a Tender Is the Beginning of the Work
A formulary listing or tender award represents access. It doesn't represent volume. The commercial work that converts institutional access into sustained revenue is harder than the work that secured the listing, because it requires coordinating clinical behavior, pharmacy operations, and field execution simultaneously.
The best institutional commercial organizations treat tender award as a trigger for intensified activity, not a signal to reduce resources. They deploy the pull-through plan immediately, monitor early dispensing data weekly, and address barriers before they become entrenched habits.
They also treat each tender cycle as preparation for the next one. The clinical evidence built during the current contract, the relationship trust developed with the pharmacy director and clinical champion, and the supply performance record accumulated over three years determine whether renewal is a competitive process or a contract confirmation.
Institutional sales is the most complex channel in pharmaceutical commercial operations. It's also, in many therapeutic categories, the highest-volume and highest-margin channel available. The organizations that invest in institutional capabilities early build defensible market positions that retail-only competitors can't easily replicate.
Learn More

Senior Implementation Consultant
On this page
- How Institutional Buying Works
- Mapping the Hospital Decision Unit
- The Tender Process Step by Step
- Formulary Listing Strategy
- Pricing Dynamics in Institutional Sales
- Why Is There a Gap Between Formulary Listing and First Order?
- Relationship Management Between Tender Cycles
- Conclusion: Winning a Tender Is the Beginning of the Work
- Learn More