Patient Awareness and Adherence Programs: Turning First-Fill into Long-Term Therapy

Turn this article into takeaways for your work.
Each assistant summarizes the article only for you and suggests best practices for your work.
Picture a patient who just received their first prescription for a chronic condition. They fill it. They start the medication. Then, ninety days later, they quietly stop. The prescriber never hears about it. The pharmacy simply stops reordering. And the rep's secondary sales numbers deteriorate while primary orders look fine.
Roughly half of patients prescribed a chronic therapy discontinue it within the first six months. Many drop off before the 90-day mark.
That gap, between a prescription written and a patient still on therapy three months later, is where most commercial teams bleed volume. Patient awareness and adherence programs exist to close it. But too many pharma commercial leaders still treat these programs as a medical affairs or marketing function rather than a field-force commercial lever. That framing is a mistake. When adherence programs are designed to be field-deployable and tied directly to secondary sales tracking and pull-through, they become one of the most reliable tools a rep team has for protecting and growing a territory.
The Adherence Cliff and What It Costs Commercially
The "adherence cliff" is the steep drop in active patients that occurs in the first one to three months of therapy. It shows up in secondary sales data as a gap between the prescription rate a territory achieves and the refill rate that follows. In chronic therapy categories such as cardiometabolic disease, respiratory conditions, and mental health, adherence rates at 12 months can fall below 50% even for well-prescribed products.
Key Facts: Patient Adherence and Commercial Impact
- Roughly half of patients prescribed a chronic therapy discontinue within the first six months, with many dropping off before the 90-day mark (PMC, 2025: https://pmc.ncbi.nlm.nih.gov/articles/PMC12429436/).
- Adherence rates at 12 months in cardiometabolic, respiratory, and mental health categories can fall below 50% even for well-prescribed products (PMC, 2010: https://pmc.ncbi.nlm.nih.gov/articles/PMC2799072/).
- Research on prescription fill rates shows an average of 73-76% of written prescriptions are actually collected by patients, meaning one in four written scripts is abandoned at the pharmacy (PMC, 2018: https://pmc.ncbi.nlm.nih.gov/articles/PMC6221733/).
The commercial consequences stack up quickly. First, each dropout is not just one lost prescription. It represents the entire remaining lifetime value of that patient's therapy, including every refill the pharmacy will no longer order. Second, if non-adherence is widespread, prescribers gradually lose confidence in the product's real-world effectiveness. They see patients who "tried it but stopped" and begin to question whether the therapy works, even when the clinical evidence is strong. That prescriber doubt is far harder to reverse than a refill gap.
Third, pharmacies respond to low refill rates by reducing their stock commitments. When a pharmacy repeatedly sees patients fail to return for refills, the pharmacist adjusts ordering to avoid carrying dead inventory. The result is a downward cycle: fewer patients refilling, lower pharmacy stock levels, occasional stockouts, and patients who do return for a refill not finding the product, leading to further dropout.
A well-designed adherence program interrupts this cycle at its earliest point. The next question is how to structure the program so it actually creates pull-through rather than just adding cost.
How Do Patient Programs Create a Pull-Through Engine?
Think of the adherence program as the connective tissue between the health care professional (HCP) relationship and the pharmacy relationship. The First-Fill-to-Refill Conversion Loop is the framework that makes this visible: a prescriber writes a script with support resources attached, the patient fills it with clear expectations set, returns to the pharmacy for refills, and the pharmacist's consistent reorder volume validates the prescriber's original choice, giving the rep adherence data for the next detail call. When the program works:
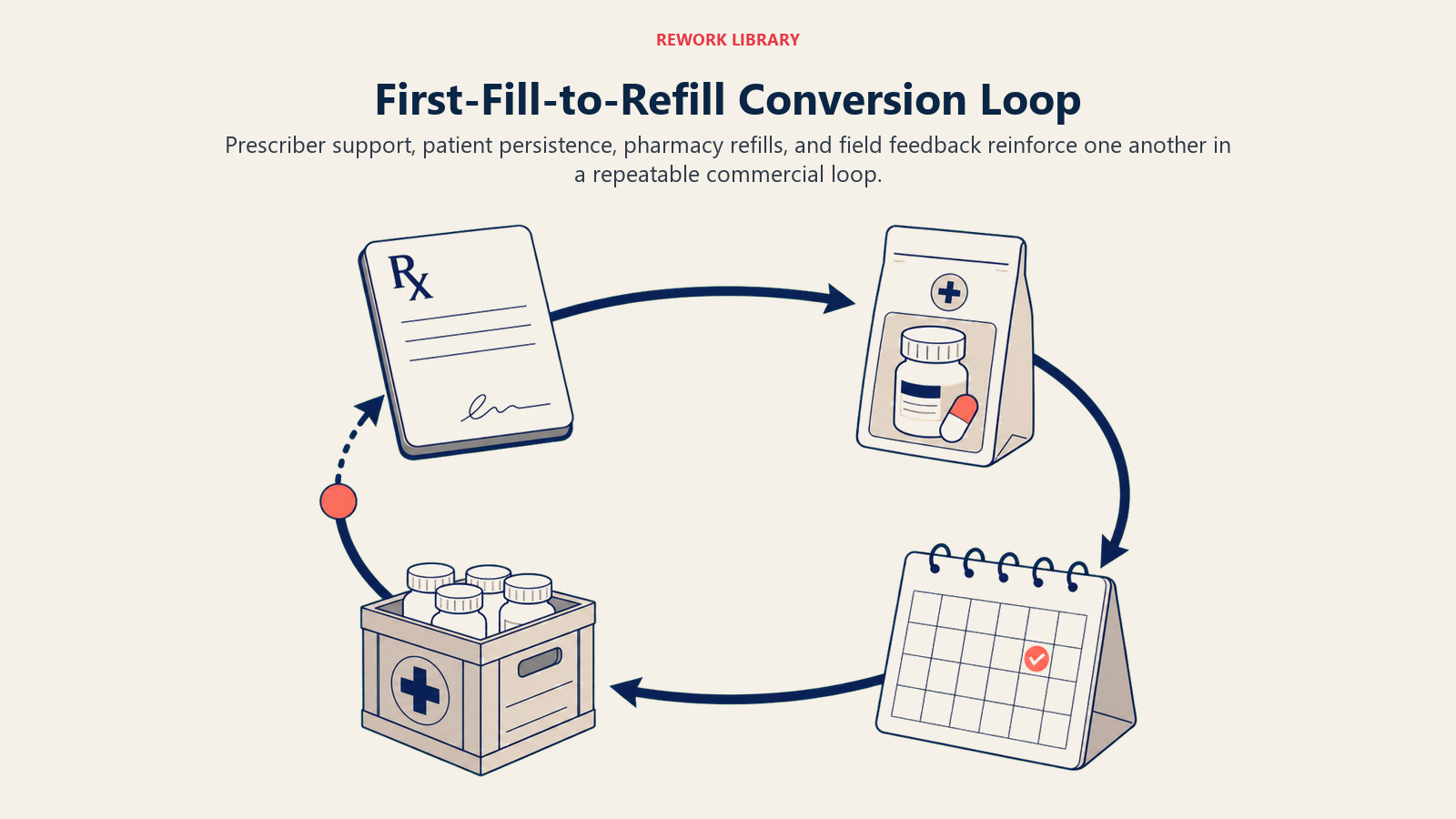
- The prescriber writes the script with confidence, knowing support resources exist for the patient.
- The patient fills the prescription, receives support material, and starts therapy with clear expectations.
- The patient continues on therapy and returns to the pharmacy for refills.
- The pharmacy's consistent refill orders validate the prescriber's choice and give the rep real-world adherence data to use in the next detail.
This pull-through engine ties directly into prescription-to-pharmacy pull-through alignment. The rep's job is not only to generate prescriptions; it is to ensure those prescriptions actually translate into sustained pharmacy dispensing. Patient adherence is the mechanism that drives that conversion.
When commercial teams view adherence programs through this lens, the investment calculus changes. It is not a cost of marketing; it is a cost of protecting revenue that has already been generated at the prescriber level.
Types of Patient Programs
Not all patient programs work the same way, and not all are appropriate in every regulatory environment or therapy category. Commercial teams need to understand the range of options and match program design to their specific context.
Disease awareness campaigns educate patients (and sometimes caregivers) on the condition itself, its risks, and why consistent treatment matters. These are typically non-branded or brand-agnostic and work best in markets where under-diagnosis or late diagnosis is a barrier to volume growth.
First-fill support focuses on the critical window immediately after the initial prescription. This can include welcome kits delivered through the pharmacy, pharmacist counseling prompts at the point of dispense, or patient support calls within the first 48-72 hours. First-fill support targets the period when patients are most likely to abandon therapy due to side effects, cost concern, or simple confusion about how to take the medication correctly.
Refill reminders reduce the passive dropout that occurs when patients simply forget to refill rather than making an active decision to stop. SMS reminders, app notifications, pharmacist-initiated calls, and even simple printed refill date cards inserted at dispense can meaningfully improve persistence rates.
Patient education materials address the most common reasons patients stop: side effects they were not warned about, dosing confusion, and unrealistic expectations about how quickly the therapy will work. Good patient education materials anticipate these failure points and pre-address them before the patient encounters them.
Nurse or pharmacist counseling tie-ins bring allied health professionals into the support structure. In many markets, pharmacists are the most accessible healthcare contact for patients between prescriber visits. Equipping pharmacists to have brief, structured adherence conversations is one of the most effective activities available in a pharmacy relationship management strategy.
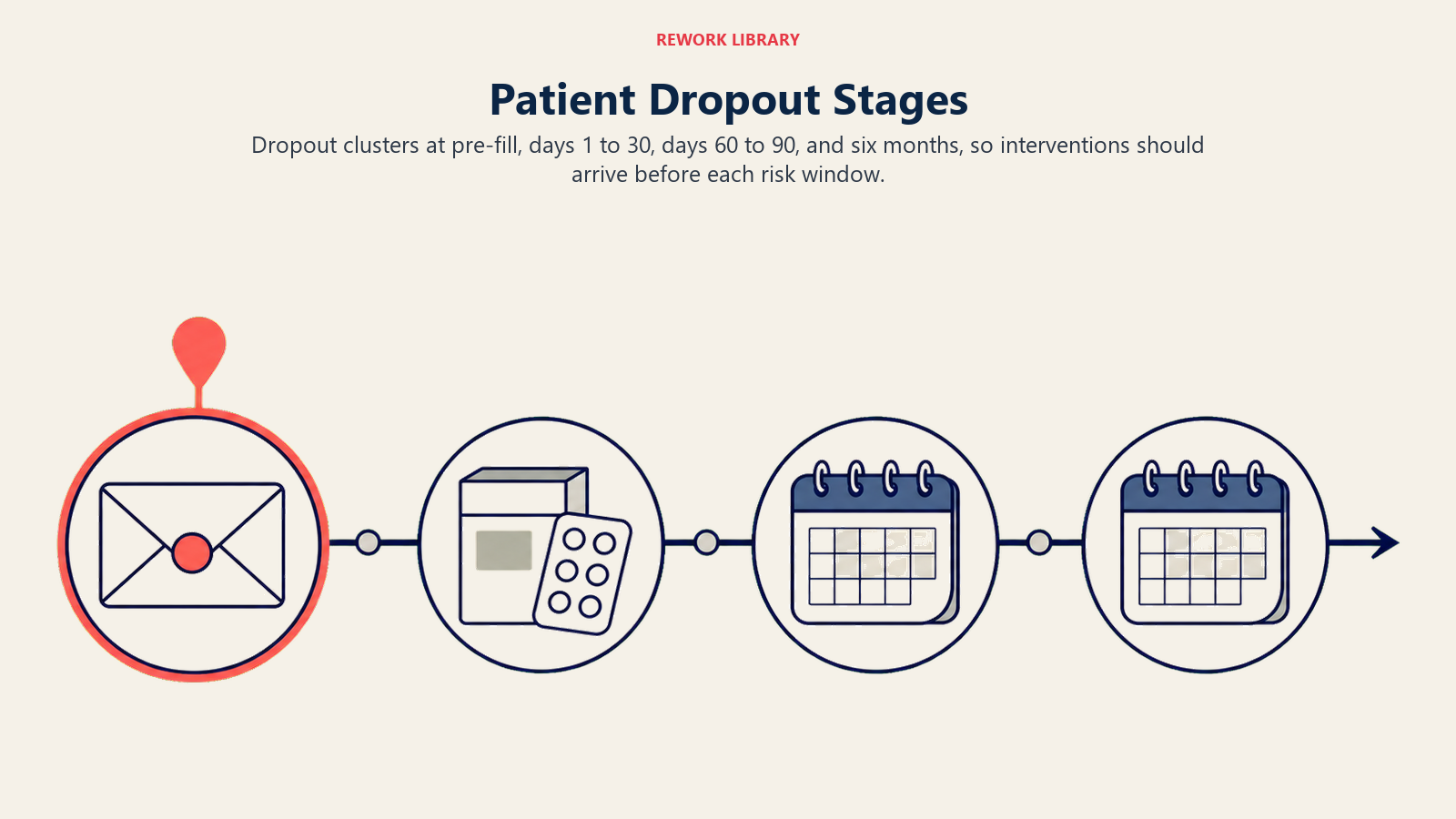
Patient Dropout Stage Map
Understanding when patients leave helps teams intervene at the right moment. Dropout typically clusters around four predictable windows:
| Stage | Timing | Primary Driver | Program Response |
|---|---|---|---|
| Pre-fill abandonment | Prescription written, first fill never made | Cost, logistics, skepticism | Copay support, first-fill outreach |
| Early discontinuation | Days 1-30 | Side effects, poor expectations | Education materials, pharmacist counseling |
| 90-day cliff | Days 60-90 | Perceived lack of benefit | Refill reminders, HCP check-in prompts |
| 6-month drop | Days 150-180 | Complacency, lifestyle change | Reactivation campaigns, repeat refill support |
The earliest interventions are the cheapest. Pre-fill abandonment and early discontinuation are where program investment delivers the best return because retaining a patient in the first 30 days costs far less than reactivating one who dropped off at six months.
Designing Field-Deployable Patient Support
One of the most common design failures in patient programs is building them entirely around central brand team delivery. The program exists as a website, a hotline number, and a brochure that reps theoretically mention. In practice, reps default to detailing the product and the program becomes invisible.

Effective programs are designed with three distinct delivery layers in mind.
Rep-deployable materials are things the rep can physically hand over during a call. This includes patient-facing brochures, first-fill cards with pharmacist instructions, refill reminder pads, and adherence tracking diaries. These materials give the rep a concrete reason to talk about adherence and give the HCP something tangible to give the patient.
HCP co-delivery materials require the prescriber or their staff to participate. This includes office-based patient counseling guides, NP or nurse scripts for post-prescription patient calls, and referral cards to pharmacist counseling services. Not all HCPs will engage with these, but for high-prescribing accounts, co-delivery can significantly improve first-fill conversion.
Centrally delivered programs run without rep involvement after the initial setup. These include SMS reminder services, patient support hotlines, and app-based tracking tools. The rep's role here is to ensure the prescriber is aware of these resources and includes them as part of the prescribing conversation, and to monitor whether program enrollment is actually happening in their territory.
Pharmacist as Adherence Ally
The pharmacist is the last professional contact a patient has before starting therapy, and often the most accessible contact if problems arise. Yet in most pharma field-force models, pharmacist interactions focus almost entirely on stock management and reordering, with little attention to the pharmacist's role in patient support.
Training pharmacists to conduct brief adherence counseling conversations is one of the most commercially valuable activities a rep can do during a pharmacy call. The conversation does not need to be long. A structured pharmacist prompt covering three points such as what to expect in the first two weeks, the most common side effect and how to manage it, and when to call the doctor can meaningfully reduce early dropout.
Connecting this pharmacist training activity directly to HCP relationship retention outcomes reveals the commercial logic: when pharmacists actively support adherence, prescribers see better real-world results and feel more confident continuing to prescribe. The pharmacist becomes an active participant in the pull-through loop rather than a passive dispenser.
Digital and Non-Digital Channels
The right channel mix for adherence support depends on the therapy area, the patient demographic, and the market's digital infrastructure. Commercial teams should resist the assumption that digital-first programs are always more effective.
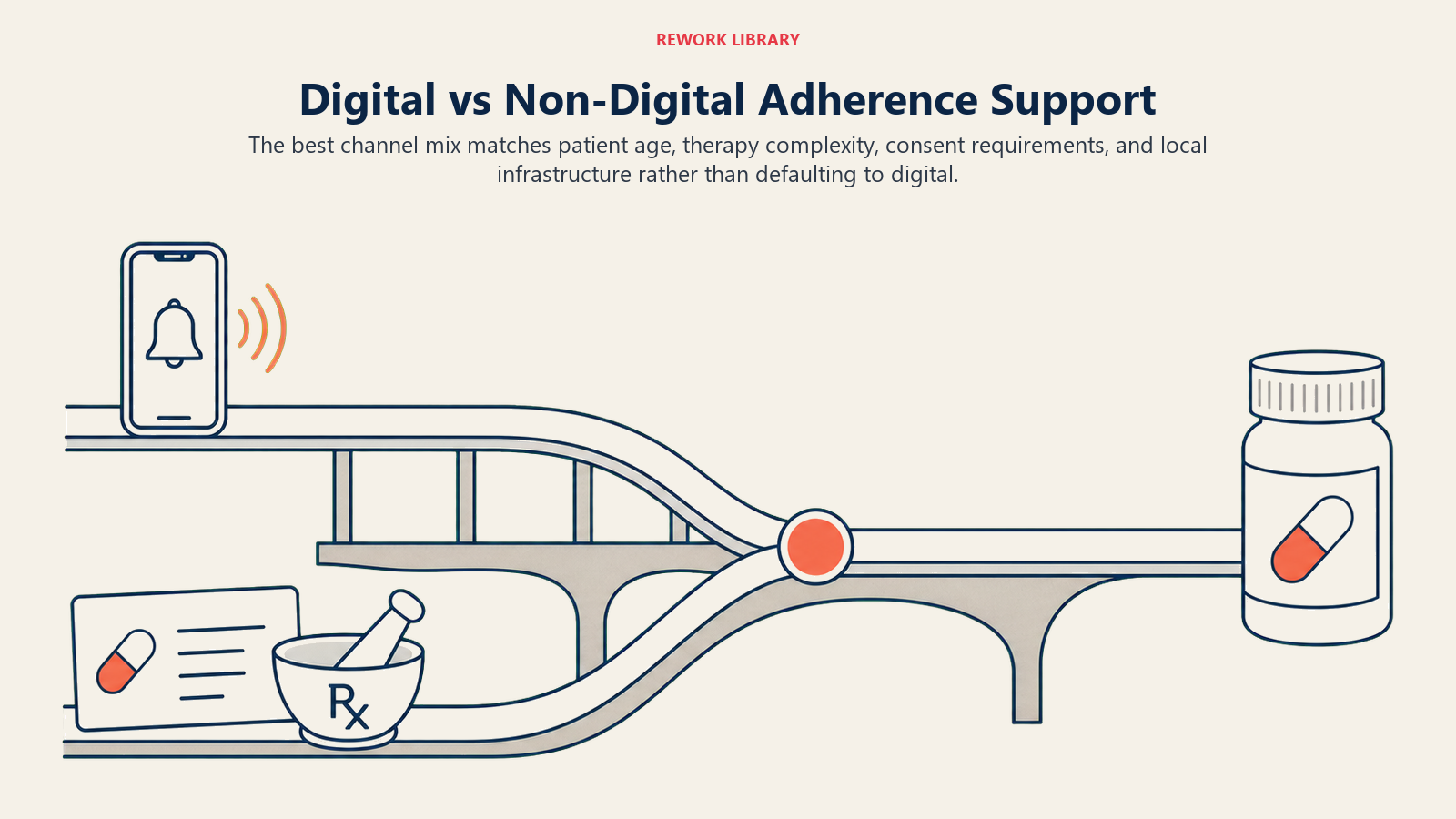
For older patient populations managing chronic conditions, printed adherence diaries, laminated dosing schedule cards, and pharmacist-assisted refill booking often outperform SMS or app-based tools. For younger patients with chronic conditions like inflammatory disease or mental health presentations, digital tools can drive strong engagement if they are simple and integrated into the patient's existing routine.
A practical framework for channel selection:
| Channel | Best Fit | Limitation |
|---|---|---|
| SMS reminders | Refill timing, appointment alerts | Requires phone number capture, opt-in compliance |
| App-based tracking | Engaged patients, complex dosing schedules | Adoption rates in general patient populations tend to be low; digital literacy and app fatigue are common barriers |
| Printed materials | All demographics, pharmacist point-of-dispense | Static, no tracking capability |
| Pharmacist counseling | First-fill support, side effect management | Depends on pharmacist willingness and time |
| Patient support hotline | High-complexity therapy, injectable products | Higher cost, requires staffing |
| Refill date cards | Low-tech, high reliability | Relies on patient retaining and acting on card |
The most effective programs combine two or three channels rather than choosing one. A first-fill card at dispense, an SMS reminder at day 25, and a pharmacist check-in at the refill window is a sequence that addresses each of the three most common dropout triggers.
Measuring Adherence Program Impact
The output metrics for adherence programs must connect back to the commercial data the field force already uses. If adherence program performance lives only in a brand team dashboard and never appears in secondary sales reporting or rep scorecards, it will remain invisible to commercial leadership and gradually lose investment priority.
The key metrics to track:
| Metric | Definition | Commercial Connection |
|---|---|---|
| First-fill rate | Percentage of prescriptions filled within X days | Baseline demand conversion |
| Refill rate (30/60/90 day) | Percentage of first-fills generating a second fill | Secondary sales predictability |
| Days-on-therapy | Average duration before discontinuation | Lifetime value per patient |
| Lapsed patient reactivation rate | Percentage of dropped patients who restart | Incremental revenue recovery |
| Pharmacist counseling completion | Percentage of first-fills with documented counseling | Adherence intervention coverage |
Connecting days-on-therapy data to secondary sales tracking metrics closes the commercial loop. When a rep can see that the accounts where pharmacist counseling rates are highest also show the strongest refill rates, the connection between patient program activity and commercial outcome becomes concrete and actionable. The same logic applies to churn prevention in subscription and recurring-revenue businesses: retaining an existing customer at the point of early disengagement costs far less than reacquiring one who has fully lapsed.
Refill Rate Tracking by Account
The table below uses illustrative targets to show how a program investment might frame account-level refill rate goals. Actual benchmarks will vary by therapy area, market, and patient population; teams should calibrate against their own historical data.
| Account Type | Illustrative Target: First-to-Second Refill Rate | Illustrative Baseline Without Program | Potential Gap |
|---|---|---|---|
| High-volume pharmacy (100+ scripts/month) | 65%+ | 45-50% | 15-20 pts |
| Mid-volume pharmacy (30-100 scripts/month) | 55%+ | 38-44% | 12-16 pts |
| Low-volume pharmacy (under 30 scripts/month) | 50%+ | 30-40% | 10-20 pts |
| Hospital outpatient pharmacy | 70%+ | 52-58% | 12-18 pts |
Gaps at high-volume accounts represent the largest absolute opportunity and should receive priority program investment.
Compliance Boundaries for Patient-Facing Materials
Patient programs operate in a tightly regulated space. Commercial teams need a working understanding of the compliance requirements before designing or deploying any patient-facing materials.
A practical compliance checklist for patient program materials:
- Program is funded and disclosed in compliance with local regulations and industry codes
- Materials do not make off-label claims or extend beyond the approved indication
- Patient personal data collected for SMS or app programs is handled under applicable privacy law (GDPR, PDPA, or equivalent)
- Pharmacist counseling scripts are reviewed and approved by medical and legal teams before field deployment
- Materials clearly distinguish between disease education content and branded product content
- Any financial assistance or copay support is structured and documented to comply with anti-kickback provisions
- Materials carry appropriate approval dates and version control
Working within these boundaries does not prevent building effective programs. But it does require that compliance review be built into the program design process from the start, not added at the end as a bottleneck. The commercial leaders who do this well treat legal and medical review as a design partner, not a gatekeeper. See pharmaceutical marketing compliance and ethics for the full regulatory framework.
Patient Adherence as a Commercial Metric
The reframe that commercial teams need to make is this: patient adherence is not a clinical outcomes metric managed by medical affairs. It is a commercial metric that determines whether the prescriptions a field force generates convert into sustained pharmacy revenue.
Every point of improvement in 90-day refill rates is a direct increase in secondary sales pull-through performance. Every percentage point of lapsed-patient reactivation is incremental revenue that requires no new prescriber acquisition. And every pharmacy that sees consistent refill volume is a pharmacy that maintains stock, reduces stockout risk, and becomes a more reliable revenue account for the rep managing that relationship.
Patient adherence programs, when designed for field deployment and measured against commercial outcomes, are among the highest-return investments a pharma commercial leader can make. The 90-day adherence cliff is predictable and preventable. The question is whether your commercial team is set up to act on it before the refills stop.
Frequently Asked Questions about Patient Awareness and Adherence Programs
What is a patient adherence program in pharmaceutical commercial operations?
A patient adherence program is a structured commercial investment designed to keep patients on therapy from first fill through long-term refills. It typically combines first-fill support, refill reminders, and patient education materials. In commercial terms, it functions as a pull-through mechanism that converts prescriptions written by HCPs into sustained pharmacy reorders.
When in the patient journey should adherence programs intervene?
The earliest interventions deliver the best return. Pre-fill abandonment and early discontinuation in the first 30 days are the most commercially recoverable failure points. Dropout at six months is significantly harder and more expensive to reverse. Programs that address cost concerns and set realistic therapy expectations before the first fill have the highest impact per dollar invested.
How do pharma reps use adherence programs during pharmacy calls?
Reps can leave rep-deployable materials such as patient brochures, first-fill cards with pharmacist instructions, and refill reminder pads. They can train pharmacists to conduct structured adherence conversations at the point of dispense. And they can monitor whether centrally delivered programs such as SMS reminders are actually enrolling patients in their territory.
How is adherence program success measured commercially?
The key commercial metrics are first-fill rate, 30/60/90-day refill rate, days-on-therapy, and lapsed-patient reactivation rate. These should connect to secondary sales data in rep scorecards so that territory-level adherence program activity is visible alongside prescription volume and pharmacy reorder rates.
What compliance rules apply to patient-facing adherence materials?
Materials must not make off-label claims, must comply with local privacy law for any SMS or app data collection, and must separate disease education content from branded product content. Any financial assistance component such as copay support must be structured to comply with anti-kickback provisions. All materials require medical and legal review before field deployment.
Why do pharmacists matter so much in adherence programs?
The pharmacist is the last professional contact before a patient starts therapy and the most accessible contact if problems arise between prescriber visits. Training pharmacists to conduct a brief, structured adherence conversation covering what to expect in the first two weeks, a common side effect and how to manage it, and when to call the doctor can materially reduce early dropout at minimal cost per intervention.
Can digital adherence tools replace pharmacist counseling?
No. App-based adherence tools tend to see limited uptake in general patient populations, and SMS reminder effectiveness depends on capturing phone numbers and obtaining opt-in consent. Digital literacy barriers, app fatigue, and privacy concerns reduce real-world adoption. For older patient populations managing chronic conditions, pharmacist-assisted refill booking and printed adherence diaries consistently outperform digital tools. Effective programs combine two or three channels rather than betting on a single digital approach.
Learn More

Senior Implementation Consultant
On this page
- The Adherence Cliff and What It Costs Commercially
- How Do Patient Programs Create a Pull-Through Engine?
- Types of Patient Programs
- Patient Dropout Stage Map
- Designing Field-Deployable Patient Support
- Pharmacist as Adherence Ally
- Digital and Non-Digital Channels
- Measuring Adherence Program Impact
- Refill Rate Tracking by Account
- Compliance Boundaries for Patient-Facing Materials
- Patient Adherence as a Commercial Metric
- Learn More