Pre-Call Planning and Objection Handling: How Prepared Reps Win More at the Counter and in the Clinic

Turn this article into takeaways for your work.
Each assistant summarizes the article only for you and suggests best practices for your work.
There's a moment every field manager recognizes. A rep comes out of a pharmacy call, notebook open, looking slightly rattled. The pharmacist brought up a competitor's price point the rep hadn't seen coming. The rep gave a vague answer, the pharmacist moved on to the next customer, and the visit ended without a clear next step. Three minutes of preparation would have prevented all of it.
Pre-call planning isn't about scripting calls into stiffness. It's about walking through a door with a clear objective, a prepared mind for the two or three pushbacks most likely to come up, and a tactical plan for what success looks like today. Reps who build this habit consistently outperform those who rely on familiarity with an account and hope the conversation flows naturally.
This article gives commercial leaders and field managers a practical framework for embedding pre-call planning into daily rep rhythm, and an objection handling model that works equally well at the pharmacy counter and in the doctor's office.
Why Most Reps Skip Pre-Call Planning
Key Facts: Pre-Call Planning and Objection Handling
- A five-minute pre-call plan in the parking lot can replace far more time spent fumbling at the counter during the visit itself, making it one of the highest-return time investments in a field rep's day.
- The commonly seen objections in pharmaceutical field sales (price/co-pay, competitor preference, low patient volume, side-effect concern, formulary restriction, and no time) surface with enough regularity that a territory-level objection library can be built, tested, and shared across the team before any health care professional (HCP) rep hits the field.
- Reps who log objections consistently in CRM give managers a territory-level pattern map that can detect payer policy changes or competitor messaging shifts within days, weeks before the information surfaces in a formal brand team review.
Ask a rep why they didn't plan before a call and the answer usually lands in one of three places: not enough time between stops, they've visited this account twenty times and feel they know it, or they had the best intentions but got pulled into a phone call in the parking lot and walked through the door unprepared.
Time pressure is real. A well-managed territory might have eight to twelve calls in a day, and when driving, documentation, and lunch are factored in, preparation can feel like a luxury. It isn't.
Repetition fatigue is more subtle. Reps who've been calling on the same pharmacy or clinic for two years carry assumptions that don't get updated. They assume the pharmacist still prefers product A over product B, when the account shifted preferred formulary status three months ago. They assume the doctor's main concern is still dosing frequency, when a recent patient complaint changed her priority to tolerability. Familiarity replaces curiosity, and that costs conversions.
Overconfidence affects high performers as often as average ones. The rep who reliably gets face time with a busy cardiologist may stop doing pre-call work precisely because the relationship feels secure. But relationship access and prescription behavior are different things. A doctor who likes a rep isn't necessarily prescribing at the rep's preferred product.
The fix isn't adding another training module. It's reducing the friction of planning to a five-minute habit that fits between calls.
The Five-Minute Pre-Call Plan
The goal isn't a comprehensive account review. It's a focused mental checklist that takes five minutes in the parking lot and loads the rep with exactly what they need for the next twenty minutes inside.

1. Account history review (two minutes)
Pull the last call note. What was the outcome of the previous visit? If the pharmacist agreed to face out a product on the shelf, did it happen? If the doctor said she'd try the medication with her next appropriate patient, is there any secondary sales data suggesting she did? Open action items from the previous call are the first thing to address. Showing up aware of what you agreed to last time signals professionalism and builds trust faster than any detail aid.
Check stock levels if the system carries them. Walking in and asking about a reorder that's already been handled wastes the first two minutes of a short visit.
2. Single clear call objective (one minute)
Write one sentence: "The objective of this call is to..." Reps who enter a call with three objectives usually achieve none of them. One clear ask creates one clear conversational path. That objective might be getting a trial commitment for new patients meeting a specific profile, confirming preferred formulary tier with the pharmacist, or reviewing a patient outcome from the last sample visit. Single-objective calls are easier to execute, easier to debrief, and easier to document afterward.
3. Anticipated objection and prepared response (one minute)
Think through the one or two most likely pushback points based on what happened last time, what the account profile suggests, or what the territory trend shows. If formulary restriction came up at the last three pharmacy calls in the area, it'll come up here too. Knowing it in advance means the rep has a response ready rather than improvising under pressure.
4. Detail aid or leave-behind selection (thirty seconds)
Detail aid and visual aid usage is most effective when the rep enters with a specific panel or page in mind for this visit. Choosing the visual anchor in advance avoids the rep flipping through materials at the counter while the pharmacist serves another customer.
5. Time estimate and entry strategy (thirty seconds)
How long is this call likely to run? Is the pharmacist likely to be behind the counter or in the back? Is the doctor's schedule tight today? Knowing the available time window shapes how the rep leads the conversation. A five-minute drop-in at a busy pharmacy requires a different opening than a thirty-minute scheduled lunch with a specialist.
The Objection Library for Pharma
Commercial organizations that let objection handling happen ad hoc in the field are leaving performance on the table. A predictable set of objections surfaces across most pharma territories, and responses to them can be prepared, tested, refined, and shared across the team.

Below is a map of the six most common objections reps encounter and a structured response approach for each. The responses aren't scripts to read verbatim. They're frameworks to internalize.
| Objection | Channel | Core Response Strategy |
|---|---|---|
| Price or co-pay concern | Pharmacy, HCP | Acknowledge cost reality, pivot to co-pay card or patient support program availability, specify steps for enrollment |
| Competitor preference | HCP, Pharmacy | Ask what's working with the competitor product, acknowledge that product's strengths, then present the differentiating clinical factor that changes the comparison for a specific patient type |
| Low patient volume in indication | HCP | Ask about recent patients who went untreated or stayed on older therapy, connect profile to data on under-diagnosed patients, offer patient identification support tools |
| Side-effect concern | HCP | Listen without interrupting, acknowledge the concern is supported by data, provide the rate and severity context, present mitigation strategies or monitoring protocol used in trial |
| Formulary restriction | HCP, Pharmacy | Clarify the actual tier status (many reps accept a perception as fact), provide a prior authorization step-by-step if required, flag the patient assistance program as a bridge |
| No time | HCP, Pharmacy | Respect it immediately and without argument, ask for sixty seconds to leave one specific piece of information, and confirm the best time to return |
The price objection at a pharmacy counter and the price objection in a doctor's office require slightly different responses. At the counter, the pharmacist is thinking about the patient in front of them, and the co-pay card process must be clear and fast. In the doctor's office, the concern is often about prescribing a product the patient will abandon because of cost. The response shifts from process to outcome: what the patient assistance program looks like in practice and whether patients stay on therapy once enrolled. Reps navigating these conversations should operate within the PhRMA Code on Interactions with Health Care Professionals, which sets clear standards for how patient support program information may be presented without crossing into improper inducement territory.
The LAER Model for Objection Handling
The LAER model (Listen, Acknowledge, Explore, Respond) gives reps a sequence that avoids the two most common mistakes in objection handling: responding before fully understanding the objection, and acknowledging without actually addressing the concern. The same four steps show up across disciplines: the objection handling framework in B2B deal-closing uses an almost identical structure, and borrowing those techniques for the pharma context is legitimate because the psychology of pushback is the same whether the buyer is a procurement manager or a skeptical cardiologist.
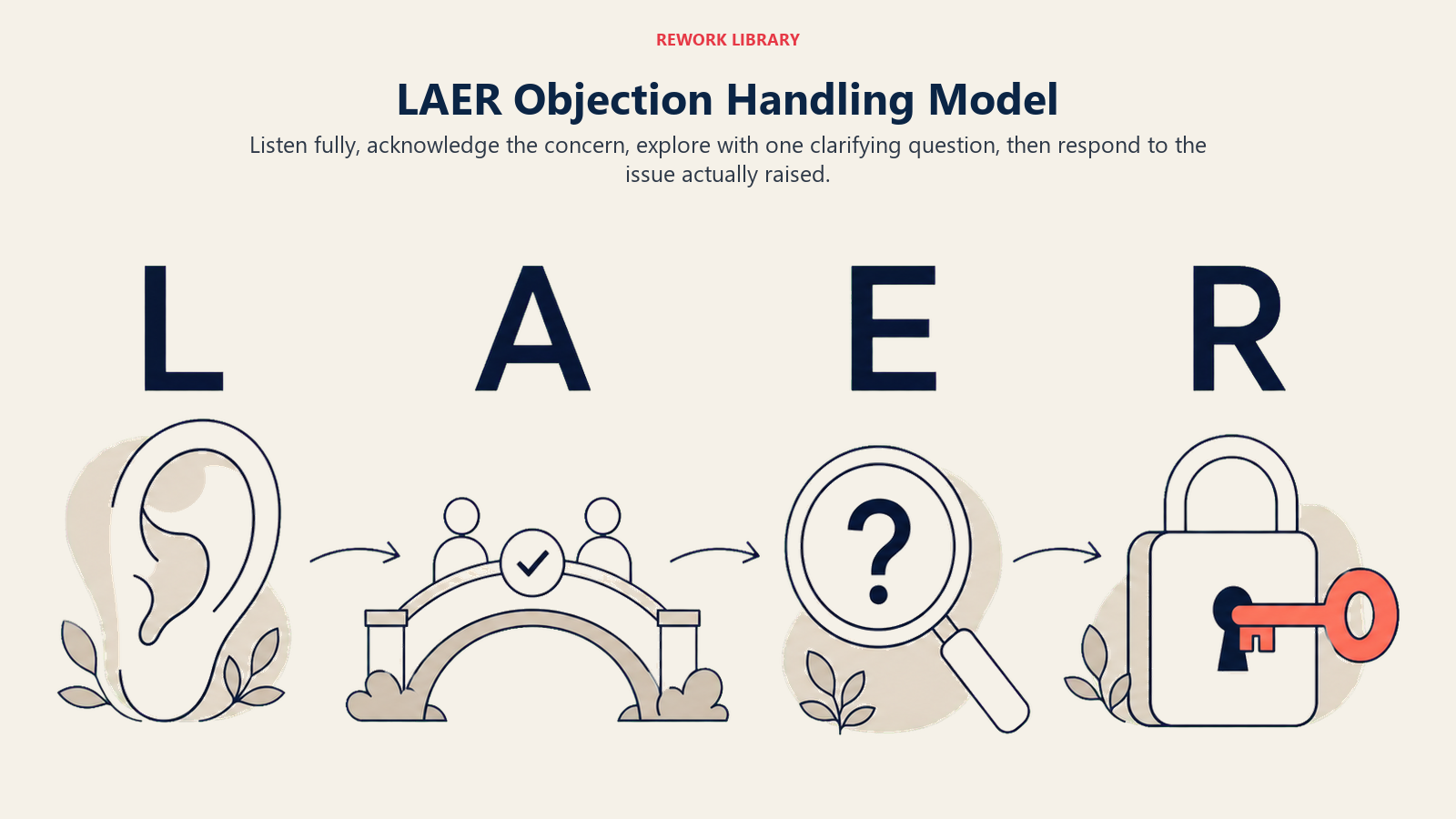
Listen: The rep stays quiet and lets the objection complete. This sounds obvious and is violated constantly. Reps who start forming their response while the pharmacist or doctor is still speaking miss information that would make the response better. A complete listen also signals respect, which changes the tone of what comes next.
Acknowledge: Before moving to any response, the rep confirms they understood what was said. "I hear you, the co-pay on this is higher than what patients are used to with a generic." Not agreement, acknowledgment. The distinction matters. Acknowledging that the concern is real and was heard creates the space for what comes next.
Explore: A question before a response. "Is the concern the sticker price or more about what patients will actually pay at the counter?" This one step filters out misread objections. A doctor who says "the side-effect profile worries me" might be thinking about a specific case from six months ago that has nothing to do with the clinical data for the broader patient population. Explore before responding.
Respond: Now the rep addresses the actual concern with a prepared and relevant answer. The response doesn't need to be long. Two or three focused sentences, tied to the specific concern the exploration clarified, outperform a comprehensive rebuttal that covers ground the other person never raised.
A concrete pharmacy example: A pharmacist says, "Patients keep asking me about switching because this is too expensive." Listen fully. Acknowledge: "You're right, the list price is higher than older alternatives." Explore: "Are most of them without insurance, or is this coming up even with patients who have coverage?" The pharmacist clarifies it's primarily cash-pay patients. Respond with the cash-pay card details and the enrollment process, not the insurance co-pay data.
A clinic example: A doctor says, "I've had a couple patients complain about GI issues with this." Listen. Acknowledge: "That's important feedback, and GI tolerability comes up in the data too." Explore: "Were these patients taking it with food or on an empty stomach?" This often uncovers a compliance issue rather than an inherent tolerability problem, and opens a clinical coaching conversation rather than a defensive product defense.
When Is the Right Time to Walk Away From a Difficult Call?
Not every call will convert on the day of the visit, and reps who push past the clear signal that today isn't the day often damage the relationship for the next visit. Recognizing those signals is a skill.
A pharmacist who answers in one-word responses while filling scripts isn't disengaged because of the product. They're under operational pressure. Wrapping the call, leaving relevant materials, and confirming a better return time is the right move. Trying to complete a five-point detail in that environment earns the rep a reputation as someone who doesn't read the room.
A doctor who says "I'm not prescribing this for my patients" after three visits and three prepared responses isn't a prospect for this quarter. The call objective shifts from conversion to information gathering: understanding what would change the calculus, so the rep returns next visit with the right new data point rather than the same tired pitch.
Walking away gracefully, with a clear next step agreed on both sides, is better detailing than staying too long. It's also better for the relationship. The HHS OIG compliance guidance for pharma manufacturers reinforces this: reps who push past a clear "no" in ways that could be perceived as coercive create compliance exposure that no conversion is worth.
Logging Objections in CRM
Every objection heard in the field is data. Reps who log objections in their pharma CRM and sales force automation system build a territory-level pattern map that managers and commercial teams can use. But the log is only useful if the underlying data is clean: inconsistent rep notes, duplicate account entries, or missing call outcomes turn an objection map into noise. CRM data hygiene practices that keep the underlying records accurate are what make objection analysis reliable at scale.
When objection logging is consistent, patterns emerge that individual reps miss. If fifteen accounts in a district are raising the same formulary restriction concern in the same week, the issue may not be individual account dynamics. It could signal a payer policy change the brand team needs to know about, or a competitor rep who's ahead of the field team with new messaging.
The log entry doesn't need to be long. Objection type, the rep's response, and the call outcome. Three fields. Over ninety days, those entries become a territory-level view of where deals are stalling and why.
Manager Coaching Application
Pre-call planning and objection handling are the two competencies where manager coaching has the highest return on investment per hour spent. Both are skills that degrade without reinforcement and improve quickly with specific feedback.
Rep onboarding, training, and coaching programs that embed objection handling practice in role-play scenarios are more effective than classroom modules, because the resistance and pressure of a realistic scenario build the muscle memory that makes the LAER sequence automatic under real-world conditions.
Managers reviewing call recordings should flag two things specifically: did the rep listen to the full objection before responding, and did the rep explore before responding? These two steps are the most commonly skipped, and fixing them produces the fastest visible improvement in call quality.
Field ride-along debriefs are most valuable when they're done in the parking lot immediately after the call, while the objection is fresh. "What was the concern the pharmacist raised? What did you hear first, and how did you check your understanding before responding?" Five minutes of immediate debrief is worth more than a formal coaching session a week later.
Reps who build a single-objective pre-call habit, one sentence before every call stating exactly what success looks like today, consistently outperform those who enter calls with multiple goals, because one clear ask creates one clear conversational path and one measurable outcome to debrief against.
Objections should be viewed as intelligence, not resistance. A pharmacist or HCP who raises a formulary restriction concern, a competitor price advantage, or a side-effect worry is revealing exactly what would need to change for a prescribing decision to happen. The rep who logs that information and returns with a precise response to the exact concern is the one who converts previously stalled accounts.
The LAER Objection Handling Model is the four-step sequence described in this article: Listen (let the objection complete before responding), Acknowledge (confirm that the concern was heard, without implying agreement), Explore (ask one clarifying question before responding), and Respond (address the actual concern the exploration revealed, not a generalized version of it). The model prevents the two most common objection-handling failures: answering before fully understanding the concern, and acknowledging without actually resolving it.
Conclusion: Planning Three Minutes Before Saves Thirty Minutes After
A rep who gets ambushed by an objection they should have seen coming spends the drive to the next account replaying the conversation, second-guessing their response, and arriving at the next call distracted. Three minutes of pre-call planning eliminates most of that cognitive cost.
The commercial organizations that outperform their peers in field productivity aren't those that hire better reps. They're the ones that build systems that make preparation habitual, make objections predictable, and make recovery fast when a call doesn't go as planned. Pre-call planning and a solid objection library are two of the lowest-cost, highest-return investments in field force effectiveness available to commercial leadership. Build that habit at the rep level and measure it at the manager level, and the returns compound every quarter.
Learn More

Senior Implementation Consultant
On this page
- Why Most Reps Skip Pre-Call Planning
- The Five-Minute Pre-Call Plan
- The Objection Library for Pharma
- The LAER Model for Objection Handling
- When Is the Right Time to Walk Away From a Difficult Call?
- Logging Objections in CRM
- Manager Coaching Application
- Conclusion: Planning Three Minutes Before Saves Thirty Minutes After
- Learn More