KOL Identification and Recruitment: Building a Key Opinion Leader Network that Drives Prescribing Influence

Turn this article into takeaways for your work.
Each assistant summarizes the article only for you and suggests best practices for your work.
One credible key opinion leader (KOL) speaking at a regional continuing medical education (CME) event can shift the prescribing behavior of a room full of attending doctors. That's not an aspirational claim. It's a pattern pharma commercial leaders see play out repeatedly in the field. A respected cardiologist describing her own clinical experience with a new antihypertensive carries more weight in that room than six months of rep visits to those same doctors.
Systematic KOL development is a force multiplier for the field team. But most pharma companies approach it reactively: they find a few physicians willing to speak, put them on a bureau list, and call it a KOL program. That's not a program; that's a speaker roster. A real KOL strategy starts with rigorous identification, moves through structured profiling, and builds a tiered network that sustains credibility across national, regional, and local levels simultaneously.
This article covers how to build that network from the ground up.
What Makes a KOL in Pharma
Key Facts: KOL Influence and Reach
- A respected specialist presenting at a regional CME event can reach 30 to 80 attending physicians in a single session, an illustrative range that shows the scale advantage over individual rep calls. Peer-delivered clinical content carries credibility that rep detailing cannot replicate one-to-one.
- The CMS Open Payments database (Sunshine Act) reported $12.59 billion in total payments and ownership interests in program year 2022, including general payments, research payments, and ownership interests across physicians, non-physician practitioners, and teaching hospitals.
- KOL programs that show measurable post-event prescribing change in attendees (tracked at 90 days) deliver a return that commercial leadership can defend, while programs with no post-event conversion tracking are increasingly the first budget line cut during downturns.
Not every high-prescribing physician is a KOL. And not every doctor who speaks at conferences qualifies either. A true key opinion leader in the pharmaceutical context has a distinct combination of attributes that translate into peer influence.
The core criteria most commercial and medical affairs teams use:
Academic or hospital affiliation and publishing record. A physician on staff at a major teaching hospital or university medical center carries institutional weight. Published research in peer-reviewed journals adds scientific credibility. The combination of affiliation plus authorship signals that peers take this doctor's clinical opinions seriously, not just their clinical practice.
Peer network reach in the relevant specialty. This is harder to measure but arguably more important. A KOL who trained dozens of fellows, chairs a major specialty society committee, or regularly presents at national conferences has a network that amplifies any message they deliver. Reach within the right specialty matters more than broad general fame.
Conference speaking history. Physicians invited to present at national meetings, serve as panel chairs, or moderate symposia have already been vetted by their peers as credible voices. Conference speaking history is one of the most reliable signals of KOL status.
Prescribing volume and product experience. This is especially important for commercial programs. A KOL who has treated substantial patient volumes in the relevant therapeutic area speaks from clinical experience, not theory. If they've used the brand and seen outcomes, that authenticity comes through in peer conversations.
Willingness to engage with industry on appropriate terms. Not every respected physician will engage with pharma, and that's their right. A KOL who won't engage is irrelevant to a commercial program regardless of their scientific standing. The practical KOL pool is physicians who are willing to participate under compliance-compliant frameworks.
KOL Tiers: National, Regional, and Local
One of the most common structural mistakes in KOL programs is treating all KOLs the same. A national thought leader in oncology shouldn't be deployed the same way as a respected community oncologist, and trying to force that fit creates inefficiency on both sides.
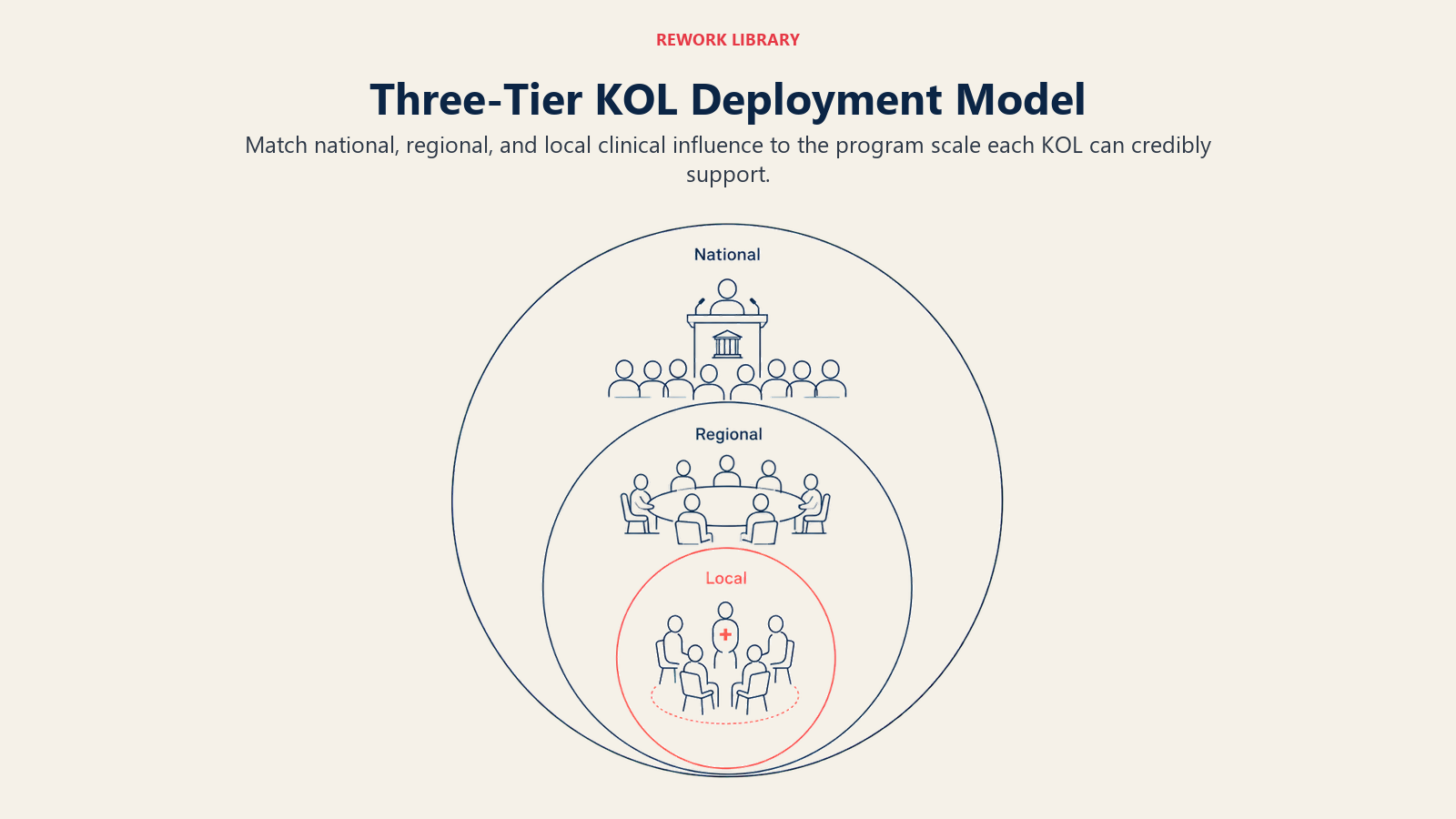 The Three-Tier KOL Deployment Model is the structural framework most effective KOL programs use: national KOLs shape scientific strategy and headline major congress events, regional KOLs drive peer-to-peer conversion at the territory level, and local champions create the face-to-face influence that moves individual prescribers in single-clinic or small hospital networks. A tiered structure matches the KOL's reach to the appropriate program type:
The Three-Tier KOL Deployment Model is the structural framework most effective KOL programs use: national KOLs shape scientific strategy and headline major congress events, regional KOLs drive peer-to-peer conversion at the territory level, and local champions create the face-to-face influence that moves individual prescribers in single-clinic or small hospital networks. A tiered structure matches the KOL's reach to the appropriate program type:
| Tier | Profile | Primary Engagement Types |
|---|---|---|
| National KOL | Major academic affiliation, national conference speaker, published researcher, clinical trial investigator | Advisory boards, clinical trial participation, national congress symposia, peer-reviewed publication support |
| Regional KOL | Regional academic or hospital affiliation, regional conference presence, recognized within a multi-state or major metro geography | Regional CME events, peer-to-peer programs, hospital grand rounds presentations, regional advisory panels |
| Local Champion | High-prescribing community physician, practice-level opinion leader, respected within a single city or district | Rep-led peer dinners, local hospital rounds, in-office peer meetings, territory-level speaking engagements |
National KOLs require medical affairs-led engagement and higher compliance scrutiny. They're typically involved in shaping clinical and scientific strategy, not just commercial programs. Regional KOLs bridge the gap between national credibility and territory-level impact. Local champions are where field teams can have the most direct influence, and they're often the most underdeveloped tier in most pharma KOL programs.
Where Do You Find KOLs in a Therapy Area?
KOL identification is a research process. The most reliable methods combine data sources with field intelligence:
Publication authorship and citation analysis. Medical literature databases let you identify physicians publishing in relevant therapeutic areas. Citation counts indicate how much their peers are reading and referencing their work. Tools like PubMed, Scopus, and specialty journals are starting points. For commercial teams, third-party KOL identification platforms (Veeva Link, H1, IQVIA) automate much of this analysis.
Conference speaker and chairperson lists. National and regional specialty conferences publish their program committees and speaker rosters. A physician who's been invited to present or chair sessions at major meetings has already been peer-selected as credible. This is one of the most efficient identification signals.
Medical society leadership roles. Physicians who serve on the boards of national or regional specialty societies, chair committee work, or hold elected positions are structurally embedded in peer networks. Their role means they communicate regularly with large groups of peers.
Nomination from the field team and existing KOLs. Field medical science liaisons (MSLs) and experienced reps often know who the respected voices in a territory are long before any database catches up. Peer nominations from established KOLs are also valuable: respected physicians tend to know who else in their specialty commands peer credibility.
Identification Source Checklist:
- PubMed/Scopus publication search in relevant therapeutic area
- Citation count analysis for identified authors
- National specialty conference speaker and chair lists (last 3 years)
- Regional conference program committees
- Medical society board and committee membership lists
- MSL and rep nomination process (formal, not ad hoc)
- Existing KOL peer nomination
- KOL identification platform data (Veeva Link, H1, IQVIA)
- Clinical trial investigator lists (clinicaltrials.gov)
- Hospital or health system committee leadership directories
KOL Profiling: What to Know Before You Engage
Identification tells you who might be a KOL. Profiling tells you whether they're the right KOL for your program, and how to engage them effectively.
A structured KOL profile should capture:
Clinical interests and current research. What therapeutic questions is this physician actively pursuing? A KOL whose research focus aligns with your brand's mechanism of action or patient population is a natural fit. One whose interests have moved elsewhere may not bring authentic enthusiasm to your programs.
Engagement history with the brand or competitors. Has this physician spoken for your brand before? Have they engaged with competing products? Prior engagement history shapes the nature of the relationship. A physician with existing positive experience is a different starting point than one who's been primarily engaged by a competitor.
Preferred interaction format. Some physicians prefer advisory roles where they can share strategic input. Others prefer speaking roles. Others are more interested in investigator-initiated research support. Matching engagement format to preference improves both recruitment success rates and long-term relationship quality.
Compliance exposure. Has this physician had any prior compliance-related issues with industry engagement? Most compliance databases and public disclosure registries (Open Payments in the US) let you review prior industry payments. Due diligence here protects the company as much as the KOL.
Prescribing data. In markets where prescriber-level data is accessible, understanding this physician's actual prescribing patterns in the relevant category provides important context for commercial relevance.
The Recruitment Process
The single most important rule in KOL recruitment is that the initial approach belongs to medical affairs or MSLs, not commercial. A commercial rep introducing a physician to a KOL engagement opportunity has an inherent conflict of interest that physicians recognize immediately. Medical affairs-led recruitment signals that the relationship starts from scientific exchange, not promotional intent.
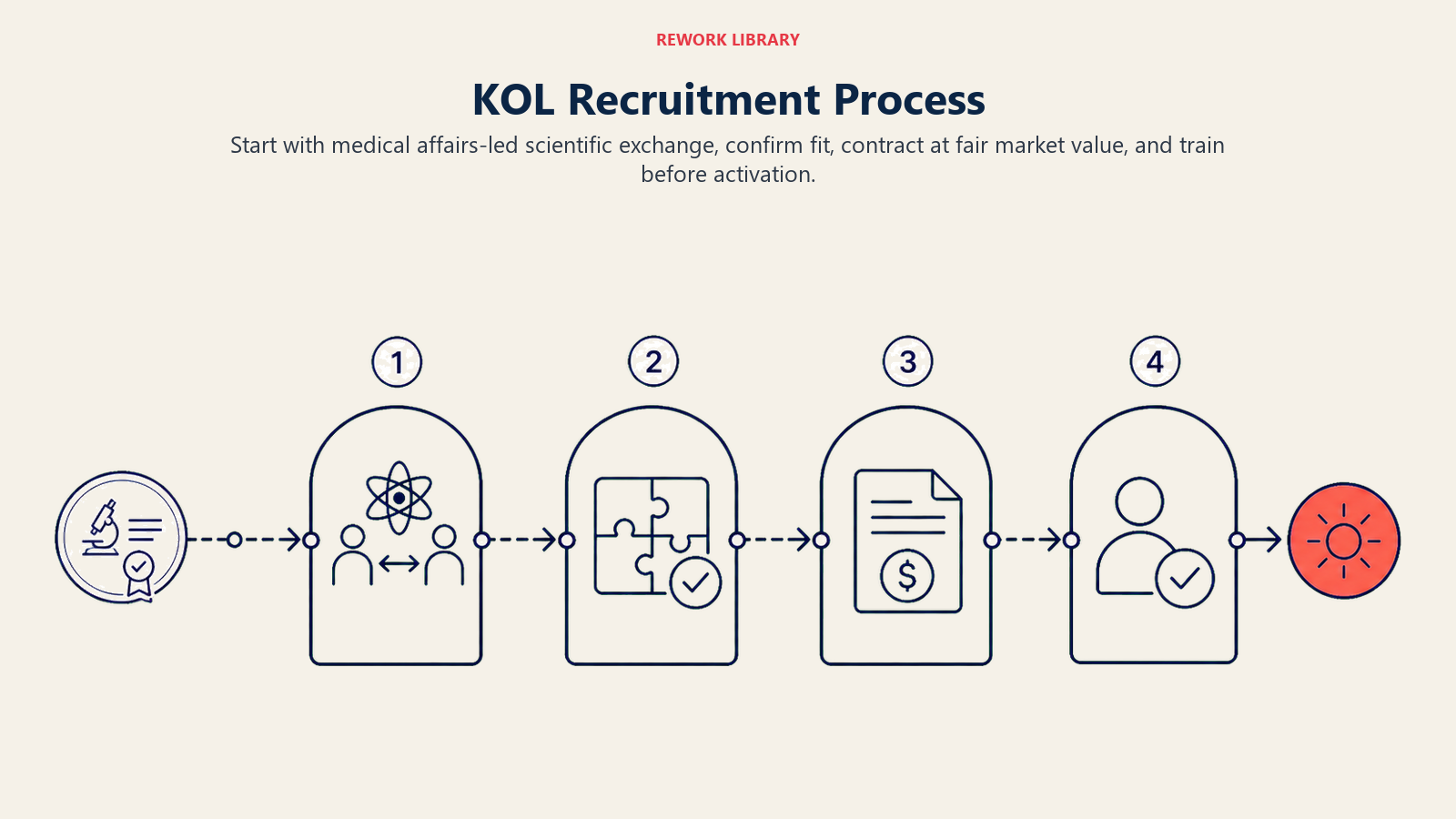 The recruitment sequence typically looks like this:
The recruitment sequence typically looks like this:
Step 1: Medical affairs or MSL initial contact. The first conversation is scientific. An MSL meets with the physician to discuss their research, share relevant clinical data, and explore their clinical experience with the relevant therapeutic area. This builds scientific credibility before any program discussion happens.
Step 2: Scoping interest and fit. If the initial scientific relationship develops positively, the MSL can begin exploring the physician's interest in advisory or educational activities. This conversation frames the opportunity in terms of scientific contribution, not commercial promotion.
Step 3: Contracting under compliance and fair-market-value frameworks. Every financial arrangement with a KOL requires a formal contract. Fair market value (FMV) for speaking fees, advisory honoraria, and travel reimbursement must be documented and defensible. Most large pharma companies use third-party FMV benchmarking tools. All contracts must comply with relevant regulations (OIG guidance in the US, EFPIA Code in Europe, local market requirements elsewhere).
Step 4: Onboarding and training. Before a KOL presents on behalf of the company, they need comprehensive training on approved messaging, on-label boundaries, and compliance requirements for speaker programs. This protects them as much as the company.
Activating KOLs for Commercial Impact
A recruited KOL who never engages creates no value. Activation is where the investment pays off, and it requires matching the engagement type to the KOL's tier and the commercial objective:
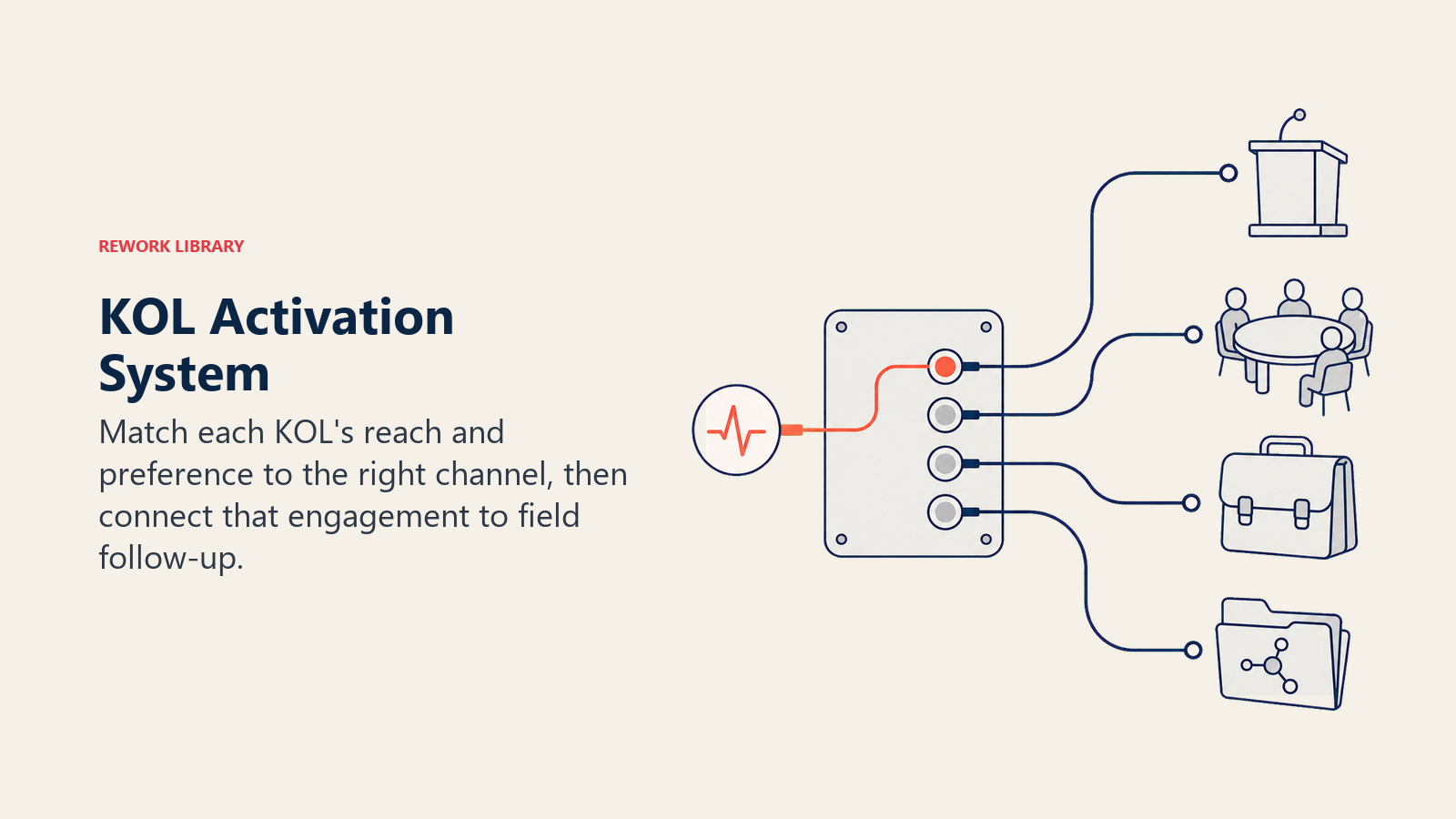 Speaker bureau programs. Regional and local KOLs delivering peer-to-peer educational events are typically the highest-volume activation channel. These programs work because peer-to-peer scientific exchange from a credible local voice carries more influence than any amount of rep detailing. Pairing speaker programs with medical education events as lead sources maximizes attendee conversion.
Speaker bureau programs. Regional and local KOLs delivering peer-to-peer educational events are typically the highest-volume activation channel. These programs work because peer-to-peer scientific exchange from a credible local voice carries more influence than any amount of rep detailing. Pairing speaker programs with medical education events as lead sources maximizes attendee conversion.
Advisory board insights. National and senior regional KOLs should have formal advisory board engagements where they provide input on clinical strategy, messaging development, and market development. Advisory inputs that genuinely inform marketing and medical strategy create a virtuous cycle: KOLs stay engaged because their input matters, and programs improve because they're shaped by credible clinical voices.
Field team co-visits for complex institutional accounts. A KOL accompanying a rep to a key academic medical center or integrated delivery network creates access and credibility that reps can't generate alone. These co-visits require careful coordination and compliance planning but can accelerate adoption in accounts that otherwise take years to penetrate.
MSL-mediated scientific exchange. Senior national KOLs often prefer to engage through medical affairs rather than commercial channels. Formal MSL engagement programs that provide clinical data briefings, support research discussions, and back investigator-initiated study proposals build the scientific foundation that commercial programs rest on. This connects directly to medical MSL and commercial alignment.
Engagement Type Menu:
| Engagement Type | Best KOL Tier | Compliance Notes |
|---|---|---|
| National CME symposium speaking | National | Speaker training required; OIG guidance applies |
| Regional peer-to-peer dinner | Regional, Local | FMV honorarium; meal cap compliance; interaction logging |
| Advisory board participation | National, Regional | FMV honorarium; input must genuinely inform strategy |
| Clinical trial investigator | National | Separate research contract; IRB oversight |
| Hospital grand rounds | Regional, Local | Often no fee for academic settings; log interaction |
| Webinar or hybrid event | National, Regional | Recording and archive compliance; off-label vigilance |
| Field co-visit | Regional, Local | Commercial-only; MSL not present; on-label only |
| In-office peer meeting | Local Champion | Small group; log all interactions; rep-facilitated |
Compliance and Transparency Requirements
KOL programs operate in one of the most heavily regulated spaces in commercial pharma. The compliance requirements aren't optional, and treating them as administrative overhead rather than strategic constraints leads to program failures and regulatory exposure.
The core requirements:
Disclosure. In most markets, KOLs who have financial relationships with pharmaceutical companies must disclose those relationships when speaking publicly. In the US, the Open Payments database (Sunshine Act) makes all company payments to physicians publicly searchable. KOLs need to understand their disclosure obligations, and companies need to support accurate reporting.
Fair market value. Every payment to a KOL, whether for speaking, advisory work, or consulting, must be documented at fair market value. FMV is determined by the physician's credentials, the nature of the work, and market benchmarks. Payments above FMV create legal exposure regardless of intent.
On-label boundaries. Speaker bureau programs and any commercial-adjacent KOL activities must stay within the approved label. Off-label promotion, even by a KOL, creates regulatory and legal liability. Speaker training, moderator oversight during events, and interaction monitoring are the control mechanisms.
Interaction logging. Every interaction with a KOL that has a commercial component needs to be logged in the CRM or relevant tracking system. This creates the audit trail that compliance and legal teams require, and it supports HCP relationship retention by giving the field team visibility into the full engagement history.
Aggregate spend reporting. Many markets require aggregate reporting of all payments to HCPs. Companies need systems that track and aggregate all KOL compensation across programs, markets, and business units for annual reporting.
Working within these constraints doesn't prevent effective KOL programs. It requires building compliance into the program design from the start rather than retrofitting it after the fact. See pharmaceutical marketing compliance and ethics for a full framework.
Measuring KOL Program Effectiveness
KOL programs are difficult to measure because the mechanism of influence (peer-to-peer scientific exchange) doesn't produce instant conversion metrics. But commercial leaders can track meaningful indicators:
 Scientific output and reach. How many presentations did KOLs deliver? How many attending physicians were reached? What's the specialty and prescribing-tier mix of the audience?
Scientific output and reach. How many presentations did KOLs deliver? How many attending physicians were reached? What's the specialty and prescribing-tier mix of the audience?
Advisory input utilization. What percentage of advisory board insights were incorporated into marketing strategy, messaging, or medical education materials? If the answer is close to zero, the advisory program is theater. Advisory boards structured as genuine listening sessions function the same way as voice of customer programs: the value is in what you do with the input, not just in having the session.
HCP conversion post-engagement. For regional and local KOL speaker programs, tracking prescribing behavior of attending physicians before and after events provides the clearest ROI signal. This requires matching event attendance records to prescribing data, which CRM integration supports. Connecting this to prescription demand generation completes the measurement loop.
KOL retention and re-engagement. High churn in the KOL network signals either poor FMV, poor program management, or KOLs who don't find the engagement scientifically meaningful. KOLs who re-engage year after year are your most valuable relationships.
Physicians who are engaged through scientific exchange before any commercial discussion is raised are more likely to remain as long-term KOL partners, because the relationship is built on professional credibility rather than transactional benefit. KOL programs that begin with a commercial pitch lose credibility with the exact doctors who have the most peer influence.
The local champion tier is the most underleveraged layer in most pharma KOL programs. A community physician who is respected within one district and speaks at a local hospital grand rounds can shift prescribing behavior among 10 to 20 peers at a cost far below regional KOL engagement, and those peers are the doctors already treating the patients in that immediate catchment area.
Fair market value documentation for KOL compensation is not just a compliance requirement. It's also a program design tool: FMV benchmarking reveals which engagement types are over-resourced relative to their peer-influence return and which are under-invested relative to their commercial impact.
Conclusion
A tiered KOL network, properly identified and engaged, creates scientific credibility that no amount of rep detailing alone can replicate. The difference between a KOL program that delivers commercial impact and one that drains budget without results usually comes down to three things: rigorous identification (not just convenience), structured profiling (so the right KOL goes into the right program), and genuine medical affairs partnership (so the relationship starts from science, not promotion).
Commercial teams that treat KOL development as a strategic priority, rather than an event-planning function, build a sustained credibility engine that outperforms their competitors across every prescriber-facing touchpoint.
Frequently Asked Questions about KOL Identification and Recruitment
What is a KOL in the pharmaceutical industry?
A key opinion leader (KOL) in pharma is a physician or healthcare professional who carries peer influence in a specific therapeutic area, beyond their own clinical practice. KOLs typically combine academic or hospital affiliation, a published research record, conference speaking history, and active engagement within specialty networks. The defining characteristic is peer trust: a KOL's clinical opinion shapes how other physicians think about a disease area or treatment, which is what creates commercial value beyond their own prescribing volume.
How do you identify KOLs at the local and regional level?
National KOLs are relatively easy to identify through publication databases and conference rosters. Regional and local KOLs are often best identified through MSL and rep nomination processes, peer referrals from existing national KOLs, and field observation of who is respected within specific hospital or clinic networks. A physician who regularly leads departmental discussions, who other doctors call for clinical questions, or who trains junior residents is a local KOL regardless of whether they appear in any formal database.
Should commercial or medical affairs lead KOL recruitment?
Medical affairs should own the initial KOL recruitment conversation, and this is a non-negotiable in well-run programs. A commercial rep approaching a physician about becoming a paid speaker carries an inherent conflict of interest that damages the relationship before it begins. Medical affairs engagement that starts from scientific exchange builds the credibility foundation that commercial programs then work on top of. After the scientific relationship is established, commercial can appropriately involve the KOL in promotional speaker bureau programs, advisory inputs, and field co-visit activities.
How do you measure KOL program effectiveness?
The clearest ROI signal is post-event prescribing change among physicians who attended KOL-led events, measured against a matched control group of non-attendees over 90 days. Secondary metrics include scientific output reach (presentations delivered, audience size by specialty), advisory input utilization rate (what percentage of advisory recommendations were incorporated into program design), and KOL retention (re-engagement year over year). Programs that cannot show prescribing change data for regional and local KOL events should build that tracking infrastructure before expanding event frequency.
What compliance requirements govern KOL speaker programs?
US KOL programs must comply with OIG guidance on speaker programs, PhRMA Code meal and interaction standards, and Sunshine Act (Open Payments) disclosure requirements. All speaker fees must be at documented fair market value, and FMV rate cards must be approved by compliance before any contracts are issued. Speaker presentations require MLR (medical-legal-regulatory) review and approval before delivery. The OIG's 2020 Special Fraud Alert on speaker programs explicitly identified circumstances that create anti-kickback exposure, including programs with high meal costs, repeated engagements of the same speakers, and attendee lists skewed toward high-prescribers.
How do KOL programs interact with the broader demand generation strategy?
KOL programs function as a demand generation multiplier: they convert the attending physician audience at speaker events into warm leads for rep follow-up, and they build scientific credibility for the brand that makes individual HCP detailing more effective. The connection only works when event attendance data flows into the CRM before the event ends, so reps can follow up within 48 hours of a KOL program with attendees from their territory. KOL programs run in isolation from field follow-up infrastructure generate awareness without conversion.
Learn More

Senior Implementation Consultant
On this page
- What Makes a KOL in Pharma
- KOL Tiers: National, Regional, and Local
- Where Do You Find KOLs in a Therapy Area?
- KOL Profiling: What to Know Before You Engage
- The Recruitment Process
- Activating KOLs for Commercial Impact
- Compliance and Transparency Requirements
- Measuring KOL Program Effectiveness
- Conclusion
- Learn More