Medical Education Events as Lead Source: Turning CME and Speaker Programs into a Prescriber Pipeline
Turn this article into takeaways for your work.
Each assistant summarizes the article only for you and suggests best practices for your work.
A well-run continuing medical education (CME) event puts a room full of relevant healthcare professionals together for a few hours. Most field teams leave without a structured follow-up plan. They send one email, maybe make a call a week later, and then treat the event as brand awareness done. The teams that convert attendance into prescriptions do something different: they treat the event as a pipeline moment before anyone walks through the door.
The shift isn't complicated. It requires field leaders to apply the same prospecting rigor to medical education events that they apply to territory coverage: who's attending, which of those attendees are in-territory, what's their current prescribing status, what follow-up should happen within 48 hours, and how do we track the conversion over the next 90 days. When that system is in place, medical education events become one of the highest-density lead-generation channels in the field force toolkit.
Types of Medical Education Events
Key Facts: Medical Education Events
- The ACCME accredits over 1,500 CME providers in the US, making structured medical education events widely available across specialties as prospecting venues for pharma field teams.
- Research on lead response time consistently shows that speed of follow-up matters significantly. The Harvard Business Review study found that companies contacting leads within an hour were nearly 7x more likely to qualify them than those waiting 24 hours or more, and the same decay pattern applies to event follow-up.
- Company-sponsored speaker dinner programs that include a structured 48-hour follow-up protocol convert a substantially higher share of in-territory attendees than programs with no formal follow-up cadence. The specific delta varies by territory and event type, but the pattern is consistent enough that 48 hours has become a standard field force operating norm.
Not all medical education events offer the same pipeline opportunity. Understanding what each event type delivers helps field leaders prioritize resources and set the right expectations for field team behavior. In the US, CME quality is governed by ACCME accreditation standards, which apply to organizations offering continuing medical education rather than to individual events.
| Event Type | Typical Attendance | Lead Quality Indicators | Primary Pipeline Use |
|---|---|---|---|
| National and regional CME conferences | 200-2,000+ HCPs | Specialty-filtered, actively seeking clinical education | High-reach key opinion leader (KOL) identification and broad awareness; follow-up pipeline for regional reps |
| Company-sponsored speaker programs | 10-30 HCPs | Invited by rep or KOL, in-territory, prescribing segment known | Highest conversion potential; structured as direct pipeline moment |
| Hospital grand rounds / departmental meetings | 15-60 HCPs | Institution-specific, attending because it's their department | Excellent for institutional account penetration; longer conversion cycle |
| Webinars and hybrid online events | 50-500 HCPs | Geographically dispersed; engagement level variable | Broad reach; strongest when paired with regional rep follow-up |
Company-sponsored speaker programs are the workhorses of pipeline conversion because the rep often controls the invite list and can pre-plan follow-up before the event runs. National conferences offer broader reach but require more coordination to connect event attendance to field team territory assignments. Webinars have scale but lower engagement intensity, which means follow-up messaging needs to work harder.
Why Should Pharma Field Teams Treat Medical Education Events as Pipeline?
The most important change a commercial leader can make is organizational: reframing medical education events as structured lead-generation activities rather than scientific obligations or brand-building exercises.
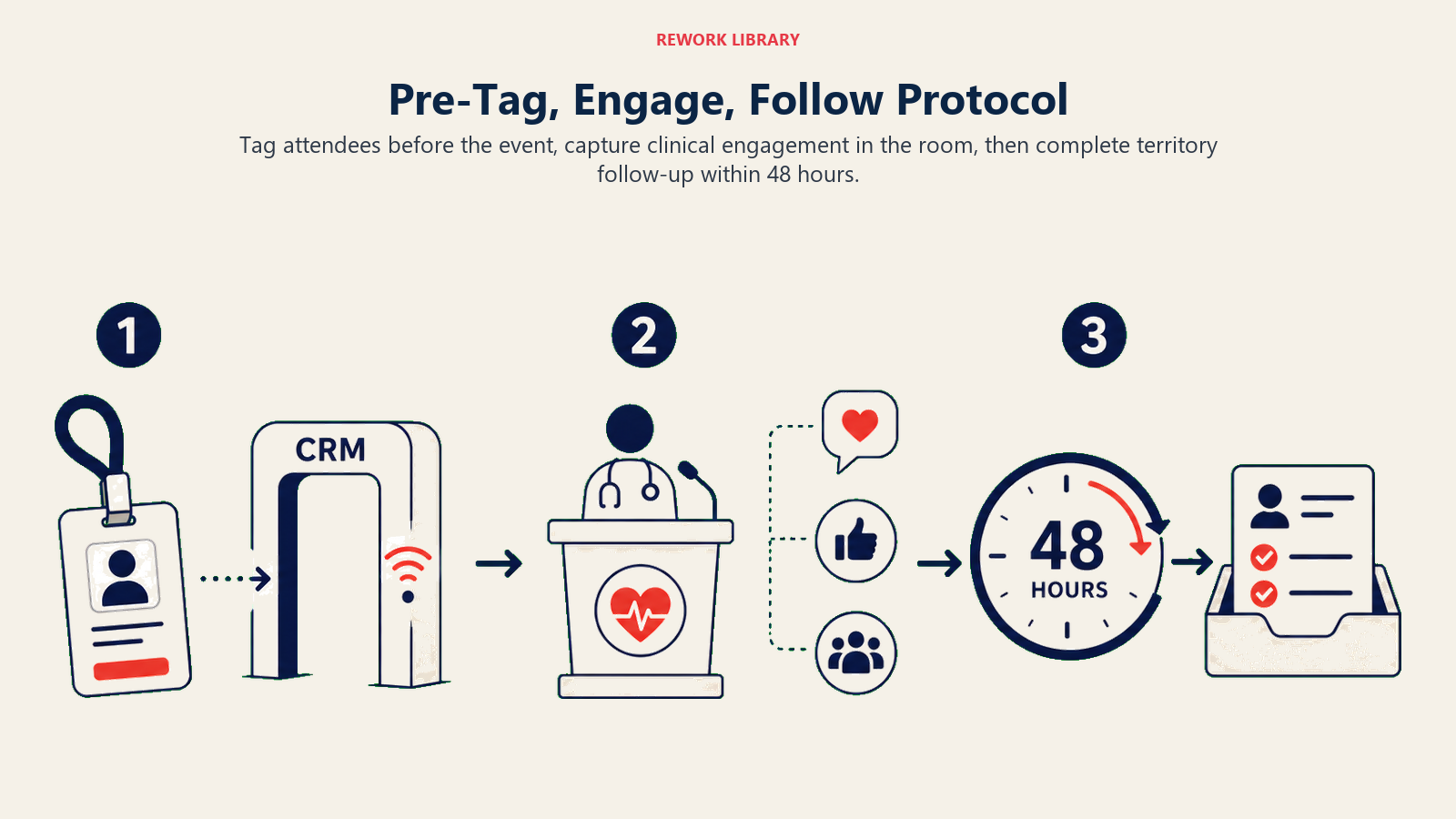
The Pre-Tag, Engage, Follow Protocol is the operating model that converts this mindset into results: pre-tag every in-territory attendee in the CRM before the event, engage with specific clinical content during the event, and follow up with a territory-relevant call within 48 hours of the event ending. Teams that execute all three steps consistently show meaningfully higher 90-day prescribing deltas than teams that execute any one or two in isolation. This reframing changes three things:
The attendance list becomes a prospect database. Every registered attendee is a potential target for the field team. The list should flow into the CRM before the event, tagged with territory assignment, current call status, and prescribing tier. Reps should know who's coming before they arrive.
The event itself becomes a qualifying touchpoint. A physician who attends a CME symposium on a specific therapeutic area is demonstrating specialty relevance and clinical interest. A physician who stays through Q and A is demonstrating active engagement with the clinical content. A physician who approaches the speaker afterward is demonstrating a level of interest that warrants prioritized follow-up. These are qualification signals, not just attendance records.
Speaker interaction becomes a KOL identification opportunity. Physicians who engage substantively with speakers, ask sophisticated clinical questions, or introduce themselves to the presenting KOL are showing peer influence within their local network. This is the frontline data that feeds your KOL identification and recruitment process. The field team is in the room; they should be watching for these signals.
Pre-Event Field Team Preparation
Most events fail as pipeline moments not because of what happens in the room but because of inadequate preparation beforehand. A rep who walks into a company-sponsored dinner without knowing which attendees are in their territory, where each stands in their call cycle, and what follow-up they've planned has already left conversion on the table.

Pre-Event Preparation Checklist:
- Pull attendance registration list at least five business days before the event
- Match attendees to territory assignments in CRM
- Pull current call status and tier for each in-territory attendee
- Pull prescribing history for each attendee where data is available
- Identify attendees not yet in the CRM as new prospect opportunities
- Brief each rep on their in-territory attendees: tier, last interaction, next objective
- Set specific follow-up targets for each rep (minimum number of follow-up calls within 48 hours)
- Pre-plan approved materials to share post-event (clinical reprints, product summary, patient resources)
- Confirm compliance setup: interaction logging plan, meal cap confirmation, approved messaging brief
- Identify any KOL networking objectives for medical affairs staff attending
The field manager's role in pre-event preparation is critical. Reps need to know this isn't optional: the attendance list is territory data, and every in-territory attendee is a lead to work.
During-Event Engagement
What the field team does during the event depends on whether it's a company-sponsored program or a third-party event. These are meaningfully different situations from both a compliance and an operational standpoint.
At company-sponsored events (speaker dinners, advisory roundtables, company-organized CME): reps typically play a hosting and coordination role. They greet attendees, ensure the program runs smoothly, make introductions between attendees and the KOL speaker, and observe engagement levels across the room. Direct selling during the scientific presentation is never appropriate. The interaction before the meal, during breaks, and after the formal program is where brief, appropriate scientific exchange can happen under the approved messaging framework.
At third-party events (national conferences, independent CME): reps are present as attendees, not organizers. Their role is relationship-building and intelligence-gathering: noting which HCPs attend which sessions, who engages with which clinical content, and who they should prioritize for follow-up. At booth or exhibit presence, reps can have substantive, compliant scientific conversations with attending HCPs.
In both settings, interaction notes should be captured the same day. Memory degrades quickly, and waiting until the end of the week to log event interactions means losing the specific clinical questions or follow-up commitments that make a follow-up conversation valuable. A brief voice note on the way to the parking lot is better than a perfectly formatted CRM entry three days later.
KOL identification during events works through observation as much as conversation. Physicians who ask clinically sophisticated questions from the floor, who are clearly known to the presenting KOL, or who draw other physicians into conversation during breaks are demonstrating peer influence. These observations should feed back into the KOL identification process through the rep's territory notes.
Post-Event Follow-Up System
The 48-hour follow-up is the highest-leverage activity in the entire event pipeline. Most of the conversion potential in a medical education event is captured or lost in the two days after it ends.
A physician who attended a dinner presentation on a new treatment option for a condition they treat regularly is thinking about that conversation right now. They may have unresolved clinical questions. They may want to see the pivotal trial data referenced by the speaker. They may want to discuss how this fits into their practice protocol. A timely, relevant follow-up catches that window. A follow-up a week later does not.
Post-Event Follow-Up Protocol:
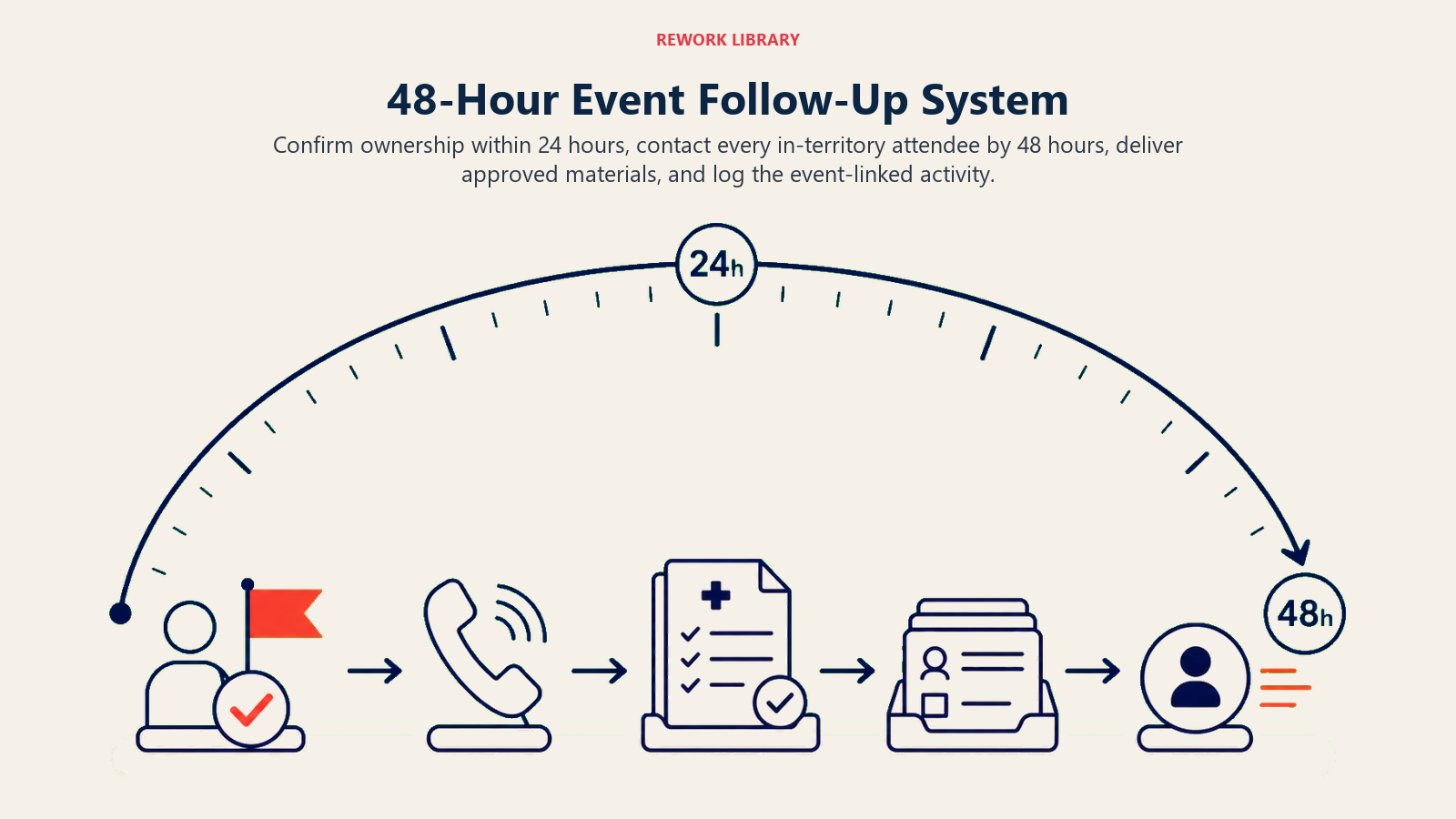
Within 24 hours: Field manager confirms with each rep which in-territory attendees they've scheduled for follow-up contact. Any attendee without a scheduled follow-up gets flagged immediately.
Within 48 hours: Each in-territory attendee receives either a follow-up call or a visit request. The opening of the follow-up connects directly to the event: "Following up from Tuesday's program on [topic]." The conversation should reference the specific content discussed, not just the event generally. Research on lead response time consistently shows that speed of follow-up matters: the physician who attended a dinner presentation is thinking about that conversation right now, and the window closes quickly. A follow-up that arrives a week later reconnects to a conversation the doctor has largely moved on from.
Materials distribution: If an attendee expressed interest in specific clinical data, a published trial, or product resources, those materials should accompany the follow-up within the 48-hour window. Pre-call planning and objection handling preparation means the rep knows which materials are approved and how to present them.
CRM logging: Every event attendee who is in-territory should have an event-linked activity logged in the CRM. This creates the data trail needed for 90-day conversion tracking and ensures that the event's pipeline contribution is visible to leadership.
New contacts: Attendees not previously in the CRM should be added as new HCP prospects immediately after the event. A physician who attended a therapeutic area event and isn't in your system is a prospecting gap the event has now identified. These feed directly into new HCP doctor prospecting workflows.
Measuring Event ROI
Medical education events carry real costs: speaker fees, venue, catering, travel, staff time, and opportunity cost. Commercial leaders who can't demonstrate return on those costs will eventually lose the budget. Measurement is how you protect and grow the investment.

Event ROI Measurement Framework:
| Metric | What It Measures | Target Benchmark |
|---|---|---|
| Attendee-to-detail conversion rate | % of in-territory attendees who receive a follow-up detail within 48 hours | Target: all in-territory attendees; flag any below 80% |
| New HCP contacts generated | Net-new HCPs added to CRM from event attendance | Track per event; benchmark to event type |
| Post-event prescribing change (90-day) | Change in target product prescriptions among attendees vs. matched non-attendees | Positive delta vs. control group |
| Cost per new HCP contact | Total event cost / new contacts generated | Benchmark against other new-contact channels |
| Follow-up call completion rate | % of planned follow-up calls completed within 48 hours | 80% or higher |
| Rep engagement score | Did reps come prepared with attendee intelligence? | Field manager observation + CRM activity data |
The 90-day prescribing delta is the metric that matters most to commercial leadership but also takes the longest to generate. Build the tracking infrastructure now, even if you won't see data for three months. Connect event attendance records in your CRM to the prescribing data feed so that the linkage is automated rather than manual.
The attendee-to-detail conversion rate and the 48-hour follow-up completion rate are leading indicators that predict the lagging prescribing outcome. If 60% of in-territory event attendees don't receive a follow-up within 48 hours, the 90-day prescribing data is going to disappoint. Fix the leading indicator, and the lagging outcome follows.
Compliance Framework
Medical education events in pharma operate under clear regulatory and industry guidelines. Getting the compliance framework right from the start protects the company, the KOL speakers, and the attending physicians.
Invitation criteria. Physician invitees should be selected based on clinical relevance to the educational content, not prescribing potential. Documentation of selection criteria should exist for every event. Blanket invitations to high-prescribers without clinical relevance documentation create compliance exposure.
Meal caps. Most markets set specific limits on the value of meals that may accompany educational events. In the US, the PhRMA Code provides guidance, and many companies set internal caps below the PhRMA ceiling. Meal value must be modest, incidental to the educational purpose, and not extended to guests or family members.
Interaction logging. Every pharma-HCP interaction that occurs during or immediately following a company-sponsored event should be logged. This is not just compliance housekeeping; it's the data that makes event pipeline tracking work. A rep who fails to log event interactions is creating a gap in both the compliance record and the commercial data trail.
Speaker fee fair market value. KOLs and physicians who speak at company-sponsored events must be paid at fair market value for their time and expertise. FMV must be documented, defensible, and consistent across similar speakers. The OIG's Special Fraud Alert on speaker programs outlines the specific risk factors regulators scrutinize when evaluating speaker compensation arrangements. See the broader compliance context in pharmaceutical marketing compliance and ethics.
Content review. All presentations at company-sponsored events require medical-legal-regulatory (MLR) review and approval before delivery. Unapproved slides, off-label content, or comparative claims that haven't passed MLR review create regulatory risk regardless of who delivers them.
Building an Event Pipeline Calendar
Medical education events become a systematic lead source when they're planned as a portfolio rather than scheduled one at a time. A field force that sees its annual event calendar in January can align territory planning, call frequency strategies, and follow-up protocols to the event schedule.
A well-constructed annual event calendar for a pharma commercial team includes:
National conference presence: Two to four major specialty conferences per year where the medical affairs team attends, KOLs present, and field teams track in-territory attendees for post-conference follow-up.
Regional CME programs: Four to eight regional events per major geographic territory, timed to quarterly business cycles and aligned to the call frequency strategy.
Company-sponsored speaker dinners: Twelve to twenty events per district per year, planned by individual reps in coordination with field managers, using local champions and regional KOLs from the bureau.
Webinar program: Monthly or quarterly webinar cadence for geographically dispersed HCPs, with regional rep follow-up built into the program design from the start.
This kind of pipeline calendar connects directly to prescription demand generation by creating regular, structured touchpoints that move HCPs along the adoption curve rather than relying on rep visits alone.
A physician who attends a sponsored dinner, stays through Q and A, and approaches the speaker at the end of the program is demonstrating stronger prescribing intent than any qualifier in a CRM scoring model. That behavior in the room is data, and reps who observe and log it walk into the 48-hour follow-up with a concrete conversation starter rather than a generic reconnect.
Medical education events are among the few commercial touchpoints where a competitor-loyal doctor might genuinely reconsider their position, because the peer-delivered clinical content carries the credibility that a rep-delivered detail cannot. An attendee who has never been called on by your brand is a warm prospect the moment they register for a relevant event.
Events that don't appear in the CRM within 48 hours of ending don't exist for pipeline management purposes. The commercial data and the compliance record both require logging, and the 48-hour window is when the conversion opportunity is highest.
Common Mistakes That Kill Event Pipeline Conversion
Understanding what breaks event pipeline conversion helps field managers prevent it:
Treating the event as the end of the activity, not the beginning. The educational program is the hook. The follow-up is where conversion happens. Field teams that celebrate a well-attended event and then move on have missed the point.
No pre-event territory matching. If reps don't know which attendees are in their territory before the event, they're not working a prospect database. They're attending a social event.
Late follow-up. A follow-up call 10 days after an event is nearly useless. The physician has moved on. The clinical questions have either been resolved elsewhere or forgotten. Forty-eight hours is the window.
Generic follow-up. "Just following up from the event" is not a follow-up. It's a check-in. A real follow-up connects to specific clinical content from the event, addresses the physician's known patient population, and advances a defined next step.
No CRM logging. Events that don't appear in the CRM didn't generate pipeline, regardless of what actually happened in the room. Field managers need to audit CRM activity after every event.
Conclusion
Medical education events are among the highest-density moments for HCP prospecting in the field force calendar. A company-sponsored dinner that puts 20 in-territory physicians in a room with a credible KOL speaker costs real money. The field teams that recover that investment treat the evening as the beginning of a structured follow-up sequence, not as the deliverable itself. The teams that don't, run the same events every quarter and wonder why the ROI never materializes.
The system isn't complicated: prepare before, engage intelligently during, follow up within 48 hours, and measure the 90-day outcome. Build that loop consistently, and medical education events become one of the most reliable pipeline-generation channels in your commercial toolkit.
Frequently Asked Questions about Medical Education Events as Lead Source
How should field teams use the event attendance list to prepare for a CME program?
The attendance list should be pulled at least five business days before the event and matched to territory assignments in the CRM. Each in-territory attendee should be tagged with their current funnel stage, last interaction date, and next call objective. Reps should enter the event knowing exactly who from their territory is attending, where each attendee stands in the prescribing pipeline, and what the planned follow-up will be within 48 hours of the event. Teams that complete this pre-work consistently convert attendance at higher rates than teams that treat the attendee list as a post-event contact export.
What's the right follow-up window after a medical education event?
Forty-eight hours is the standard. Physicians who attended a dinner presentation on a specific clinical topic are still thinking about that conversation within the first two days. Clinical questions are unresolved, prescribing protocols are under mental review, and the rep's name is still fresh. A follow-up call or visit that references specific content from the event connects directly to that active clinical thinking. A call made seven to ten days later reconnects to a conversation the physician has largely moved on from, reducing the practical impact to near zero even when the message itself is identical.
How do you track prescribing outcomes from medical education events?
Connect event attendance records in the CRM to the prescribing data feed at the HCP level. Tag each in-territory attendee with the event date and event type, then pull their prescribing data for the target product 30, 60, and 90 days after the event. Compare that to a matched control group of non-attending HCPs with similar profiles to isolate the event's contribution. This requires that attendance records be logged immediately after the event. Retroactive logging from memory misses the specificity needed for clean attribution.
What's the difference between company-sponsored speaker programs and third-party CME events?
Company-sponsored speaker programs are events the pharma company organizes, where a rep typically controls the invite list, selects the KOL speaker, and plans the follow-up. Third-party CME events (national conferences, independently organized symposia) are events the company attends but does not control. At company-sponsored programs, reps play a hosting role and can pre-plan targeted follow-up by territory. At third-party events, reps are present as attendees and their role is relationship-building and intelligence-gathering. Compliance rules also differ between the two event types, with company-sponsored events subject to stricter interaction logging and speaker fee documentation requirements.
How many company-sponsored speaker events should a district plan per year?
A planning benchmark for most pharma commercial districts is 12 to 20 company-sponsored speaker dinners per rep per year, or roughly one to two per month per district team. The cadence should align with the call frequency strategy: events work best when they're part of a systematic HCP engagement calendar rather than clustered around product launches or budget year-end. Districts that plan their event calendar in January and align it with territory coverage priorities fill rooms with higher-value attendees than teams that schedule events reactively.
Learn More

Senior Implementation Consultant
On this page
- Types of Medical Education Events
- Why Should Pharma Field Teams Treat Medical Education Events as Pipeline?
- Pre-Event Field Team Preparation
- During-Event Engagement
- Post-Event Follow-Up System
- Measuring Event ROI
- Compliance Framework
- Building an Event Pipeline Calendar
- Common Mistakes That Kill Event Pipeline Conversion
- Conclusion
- Learn More