Prescription Demand Generation: How Pharma Commercial Teams Build Sustainable Script Volume
Turn this article into takeaways for your work.
Each assistant summarizes the article only for you and suggests best practices for your work.
Distribution without demand is just inventory. A product sitting on a pharmacy shelf generates no revenue until a doctor writes a prescription and a patient walks in asking for it. Getting product into pharmacies is necessary, but it's not sufficient. The commercial teams that consistently outperform competitors understand this distinction and invest accordingly in the discipline that actually drives scripts: prescription demand generation.
Prescription demand generation is the set of activities, programs, and interventions that move healthcare professionals from passive awareness of a brand to active, habitual prescribing. It's not a marketing function or a medical affairs function in isolation. It's a coordinated commercial capability that sits at the intersection of field force execution, marketing program design, and data-driven measurement.
This article helps pharma commercial leaders understand the demand generation funnel, the levers available at the rep and marketing level, pull-through mechanics, and the measurement systems that connect activity to prescription outcomes.
Why Demand Generation Is the Engine of Field Investment Returns
Key Facts: Prescription Demand Generation
- Field force investment is substantial: rep salary, car allowance, samples, travel, and management overhead make each US medical rep one of the most expensive commercial channels a pharma company operates. See pharma field sales economics for the full cost breakdown.
- Script conversion rates for detailed HCPs in well-managed demand programs are typically higher than for unstructured detailing; rates below 20% are widely used as a signal of a call quality or targeting problem rather than a product issue.
- Sampling with a specific patient case discussion consistently produces higher conversion rates than generic sample distribution, because the sample is linked to a scripted action the doctor can take immediately.
Field investment is expensive. A single medical representative carrying salary, car allowance, sample budget, travel expenses, and manager overhead represents a substantial annual cost for a pharma company, varying by market and seniority. Multiply that across a field force of 50 or 500, and the investment is significant. (For a full breakdown of rep economics, see pharma field sales economics.)
That investment generates returns in one way: when HCPs who've been detailed write prescriptions for the products they've been detailed on. Everything else, call frequency, sample placement, leave-behind materials, is an input. Prescriptions are the output.
Demand generation programs are the mechanism that converts inputs into outputs. Without deliberate demand generation, field activities are largely sunk costs. The rep visits, the doctor nods politely, and the script habits don't change. With effective demand generation, each interaction moves the HCP a measurable step closer to trial prescribing, regular prescribing, or deepened loyalty.
This is the framing pharma commercial leaders need: demand generation isn't a campaign. It's the operational system that makes the field force investment pay back. And the system starts with understanding where each doctor sits in the adoption sequence.
What Is the Prescription Demand Funnel?
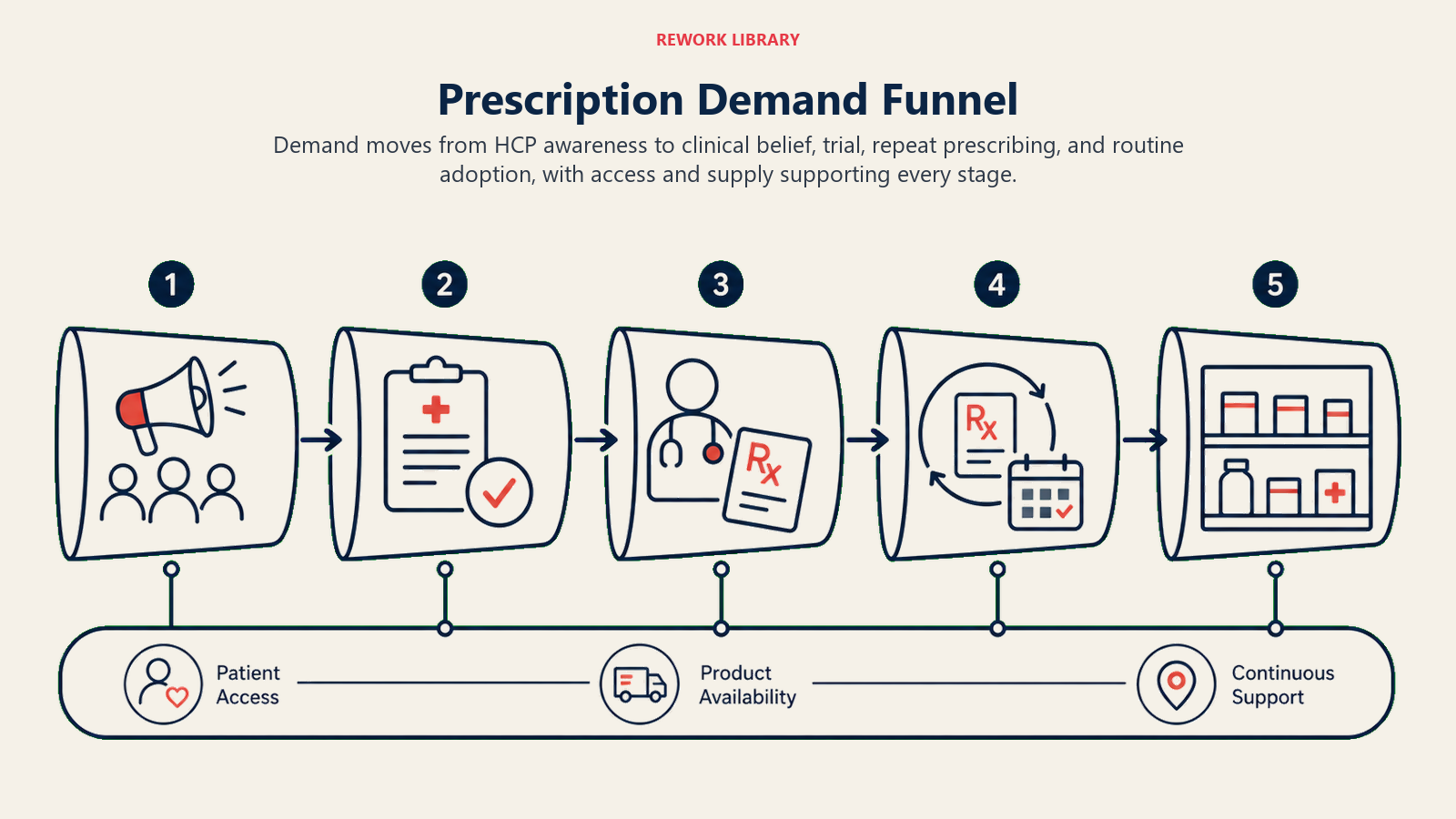
Understanding where each HCP sits in the demand funnel determines what demand generation activity is appropriate for them. Not every doctor needs the same intervention. A doctor who's never heard of your brand needs something different from one who's prescribed once and hasn't repeated.
Prescription Demand Funnel
| Stage | HCP Behavior | Demand Generation Objective |
|---|---|---|
| Unaware | Doesn't know the brand or molecule exists | Create awareness: brand name, molecule, general indication |
| Aware | Knows the brand but hasn't formed a clinical view | Build understanding: clinical evidence, patient type fit, differentiation |
| Trial | Has written 1-2 prescriptions, exploring fit | Reinforce the trial: positive patient feedback, next patient type |
| Adoption | Writes prescriptions regularly for appropriate patients | Broaden adoption: additional indications, patient volume growth |
| Loyalty | Defaults to product as first-line choice, recommends to peers | Protect loyalty, use for peer influence |
Most territories have HCPs at every stage simultaneously. A field force manager's job is to ensure the rep team is executing demand generation activities appropriate to each HCP's current stage, rather than delivering the same call content to every doctor on the list. Companies outside pharma solve the same problem with lead nurturing programs, and the structural logic transfers directly: define stages, assign stage-appropriate content, and track progression rather than just contact volume.
The Stage-Calibrated Detailing Model is the demand generation framework this funnel supports: assign every HCP in the territory a funnel stage, select the demand lever appropriate to that stage before the call, and track funnel advancement rate (the percentage of HCPs moving at least one stage per cycle) as the primary leading indicator of future prescription growth. A rep who's still presenting awareness-level content to a doctor who's already in the adoption stage is wasting both the rep's time and the doctor's attention. A rep who tries to convert a loyalty-stage message on an unaware doctor creates confusion. Stage-appropriate demand generation is what converts field activity into prescription results. The rep is where that conversion happens first.
Demand Generation Levers at the Rep Level
The medical representative is the primary demand generation vehicle for most pharma brands. The one-to-one relationship between a trusted rep and an HCP is still the most effective channel for moving doctors through the prescription funnel. But "detailing" as a generic activity isn't demand generation. Purposeful rep-level tactics make the difference.
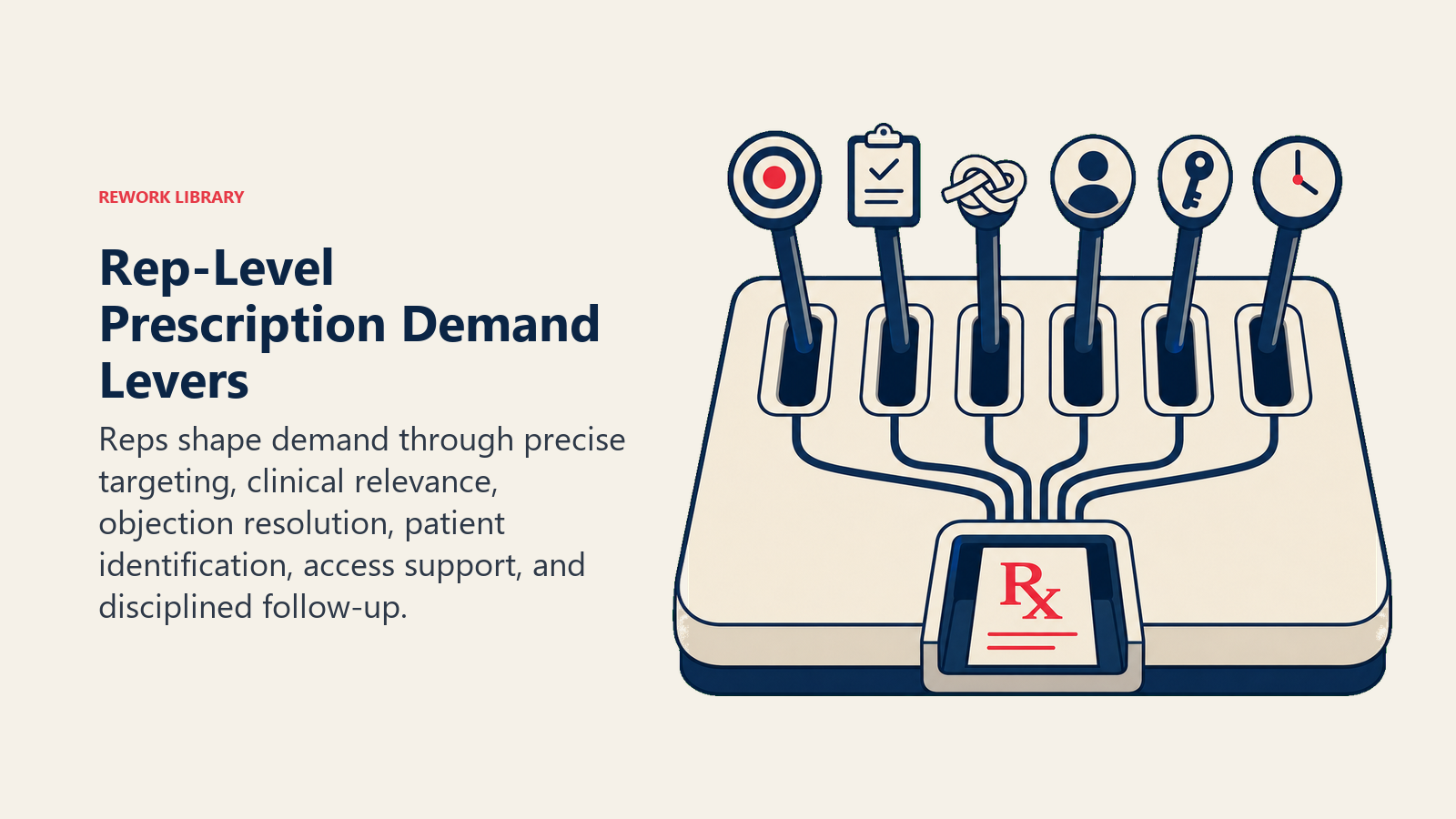
Targeted detailing focused on patient case types
Generic brand presentations don't create prescribing intent. What creates intent is helping a doctor see a specific, realistic patient in their practice who would benefit from the product. The shift from "this product treats hypertension" to "your Type 2 diabetic patients with Stage 2 CKD are the ones most likely to respond to this mechanism" is the difference between a forgotten detail and a changed prescribing habit.
Train reps to identify a patient case type in each call based on what they know about the HCP's practice profile. The question "which of your current patients fits this profile?" is more powerful than any brochure because it makes the prescribing decision concrete and immediate.
Clinical evidence delivery matched to HCP practice focus
Evidence is not one-size-fits-all. A family physician wants to see primary care trial data and practical dosing guidance. A cardiologist wants outcome data and cardiovascular safety signals. An endocrinologist wants metabolic parameters and long-term glycemic control data.
Build modular evidence delivery into your detailing system so reps can select the data most relevant to each doctor's specialty and clinical focus. A single "core message" that works for all specialties is likely to be sufficiently generic that it lands for none of them.
Sampling and starter-pack programs
Samples remain one of the most effective demand generation tools in pharma, because they reduce the prescribing risk for a doctor considering a new product. A doctor who's uncertain about a patient's response can offer a sample to bridge the gap between prescription and commitment.
But sampling without a specific patient case discussion is poor demand generation. "Here are some samples" creates no prescribing intent. "Here are samples for your next patient who presents with [specific condition], this profile has the best evidence for response" creates a scripted action plan. The difference in conversion rate between generic sample distribution and targeted sample placement is significant enough to warrant a formal protocol in your field force operating standards.
Sample-to-script conversion tracking provides the data to understand which HCPs are converting samples into prescriptions and which aren't, allowing managers to intervene with coaching or adjusted targeting.
Demand Lever Menu for Rep-Level Demand Generation
| Lever | Best Fit Stage | Execution Note |
|---|---|---|
| Brand awareness call | Unaware | Brief, introduce molecule and indication only |
| Clinical evidence presentation | Aware | Match evidence to HCP specialty, specific patient type |
| Patient case discussion | Aware to Trial | Pre-identify eligible patient type in this doctor's practice |
| Targeted sample placement | Trial | Link to specific patient case, request feedback on next visit |
| First-prescription follow-up | Trial | Call or visit within 2-3 weeks to ask about patient experience |
| Indications expansion | Adoption | Introduce second or third eligible patient population |
| Peer reference / success case | Adoption to Loyalty | Share de-identified outcomes from similar practice type |
| Key opinion leader (KOL) referral facilitation | Loyalty | Enable loyal prescriber to influence peers at continuing medical education (CME) or clinic rounds |
Marketing-Supported Demand Programs
Rep-to-doctor interaction is the most direct demand generation channel, but it has structural limits. Reps have finite call capacity, access to some HCPs is restricted, and individual rep knowledge and execution varies. Marketing-supported demand programs extend the demand generation system beyond what the field force can do alone.
Speaker programs and peer-to-peer education
Doctors are more influenced by peer clinicians than by pharmaceutical representatives, particularly on clinical decision-making. Speaker programs that enable respected clinicians to present evidence to peer audiences generate credible demand at a scale the field force can't replicate.
Speaker programs work best when the topic is directly relevant to the prescribing context of the audience, the speaker is credible in the same specialty, and the program structure enables genuine clinical discussion rather than a promotional monologue. Programs that feel like sales events generate cynicism, not prescribing intent.
Patient awareness campaigns
Patients who ask their doctors about a specific treatment by name create pull-through demand. Consumer-facing patient education campaigns that describe symptoms, encourage patients to discuss treatment options, and direct them to their doctor create a downstream demand signal that complements HCP-facing programs.
These campaigns don't require the patient to know the brand name. Condition-awareness campaigns that encourage diagnosis-seeking behavior are often as effective for driving scripts as brand-name campaigns, particularly in therapy areas where patients are underdiagnosed.
Digital content programs for remote HCPs
Reps can't call on every HCP in the territory at the frequency required to move them through the demand funnel. Digital programs, including email newsletters with clinical content, webinar-based evidence presentations, and portal-based HCP resources, extend demand generation reach to doctors with limited face-to-face access.
Digital demand programs work when the content is genuinely useful, not just promotional. An email sequence that delivers relevant clinical trial summaries, patient case studies, and prescribing guidance over 8 to 12 weeks creates more prescribing intent than a single promotional email blast.
New HCP doctor prospecting creates the pipeline that these marketing programs then work on. Prospecting identifies the doctors; demand programs convert them.
Pull-Through Mechanics: Connecting Demand to Dispensing
Demand generation creates prescription intent. Pull-through ensures that written prescriptions convert into dispensed units. The two systems need to be coordinated, or you'll generate demand that leaks at the pharmacy level.
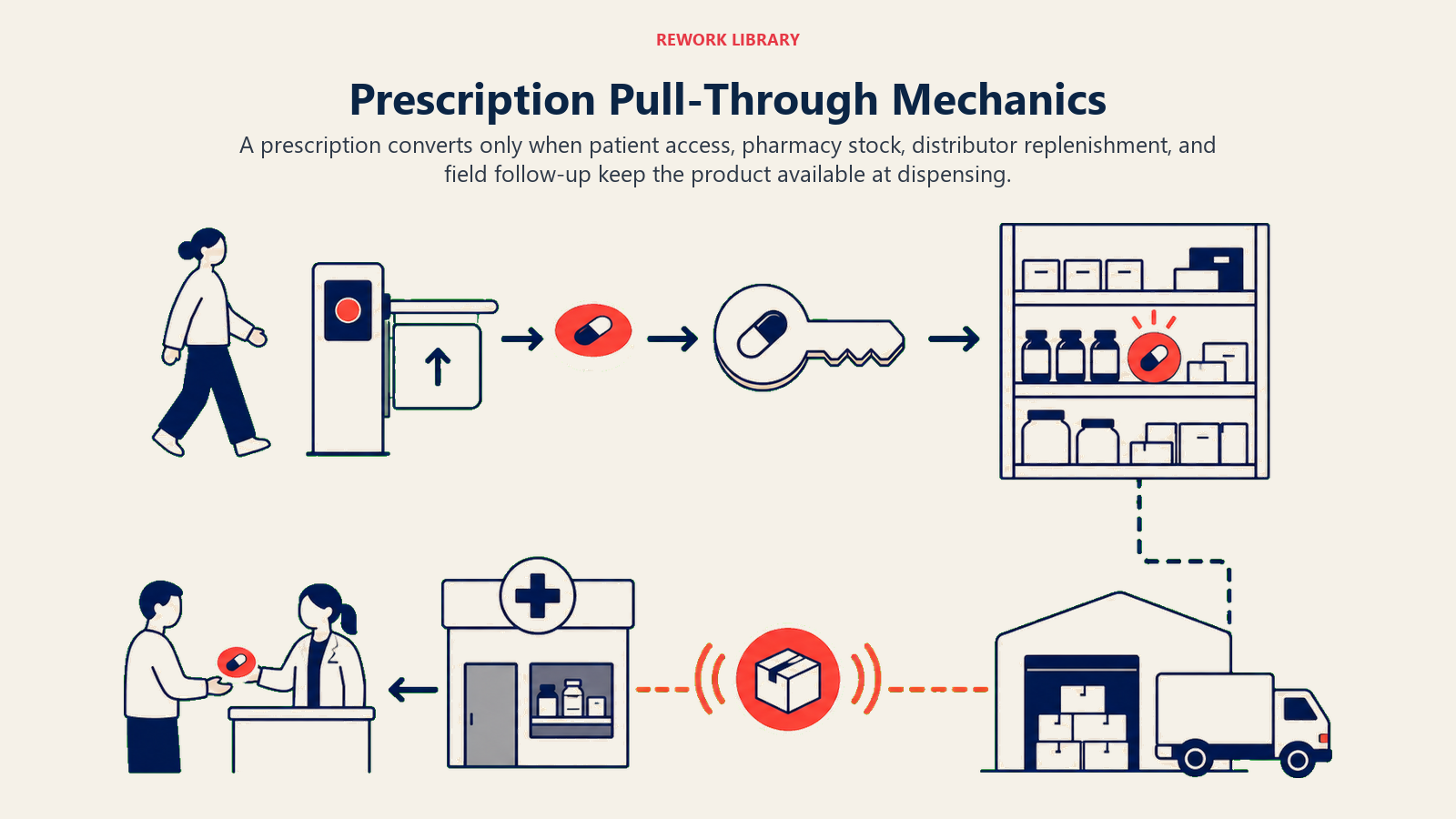
Ensuring pharmacy stock before demand is created
The sequence matters. If your HCP detailing campaign creates prescribing intent before the nearby pharmacies are stocked, the patient arrives at the pharmacy, the pharmacist can't fill the script, and the patient either waits (often too long) or accepts a substitute. That's a lost conversion even though the demand was successfully generated.
Field force coordination between HCP reps and pharmacy reps should ensure that distribution coverage in a given geography is completed before, or at minimum concurrent with, HCP demand generation efforts in that geography. A territory launch or a geographic push needs pharmacy stocking as a prerequisite, not an afterthought.
Coordinating pharmacy rep activity when doctor demand builds
When HCP detailing is creating prescription volume in a specific area, pharmacy reps should increase call frequency in nearby outlets to ensure stock levels keep pace. IQVIA or equivalent prescription data can identify pharmacy fill locations for specific products, allowing the pharmacy team to prioritize stocking visits where prescription demand is building.
This coordination between field teams requires regular communication: weekly territory reviews that share HCP activity data and pharmacy stock status across both teams. Without it, the two field forces operate as separate units that don't reinforce each other's work.
Prescription-to-pharmacy pull-through alignment addresses this coordination in detail, including the data flows and meeting rhythms that keep HCP and pharmacy activity synchronized.
Secondary sales tracking and pull-through provides the measurement framework for understanding where prescriptions are converting into pharmacy sales and where they're leaking.
Measuring Demand Generation: Connecting Activity to Script Outcomes
Demand generation programs that aren't measured against prescription outcomes are activity programs, not commercial programs. The measurement framework needs to connect rep activity data to prescription data at the HCP and territory level.

Primary Demand Generation KPIs
| KPI | What It Measures | Source |
|---|---|---|
| Script conversion rate | Percentage of detailed HCPs who wrote at least one prescription in the last 90 days | IQVIA/IMS prescription data vs. CRM call records |
| Demand velocity | Average days from first detail to first prescription | CRM call dates vs. first prescription date |
| Sample conversion rate | Percentage of sample recipients who wrote a prescription within 60 days | CRM sample records vs. prescription data |
| Funnel advancement rate | Percentage of HCPs advancing at least one funnel stage per cycle | CRM funnel stage tracking |
| Active prescriber growth | Net change in HCPs with at least one prescription per month | Monthly prescription data by HCP |
| Prescription frequency by prescriber stage | Average scripts per month by funnel stage | Prescription data segmented by CRM funnel stage |
Demand Generation Measurement KPI Table
| KPI | Planning Range | Red Flag |
|---|---|---|
| Script conversion rate (detailed HCPs) | Varies by portfolio; 20%+ for structured programs | Below 20% indicates call quality or targeting issue |
| Demand velocity (days to first script) | 45-90 days (primary care benchmark) | Over 120 days suggests weak clinical messaging |
| Sample conversion rate | Higher with targeted placement than generic distribution | Below 25% indicates untargeted sample placement |
| Funnel advancement rate per cycle | 15-20% of HCPs advance one stage | Below 10% suggests rep detailing isn't creating movement |
| Active prescriber growth month-over-month | 5-8% | Flat or declining indicates prospecting and demand gen aren't connected |
Prescription data from IQVIA or equivalent market data providers should be reviewed at the HCP level, not just the territory level. Territory-level script data masks significant variation in individual HCP performance. A territory with 100 detailed HCPs but only 15 active prescribers has a demand generation problem that aggregate territory data doesn't reveal.
Doctor detailing best practices provides the call-level execution standards that drive the activity side of these metrics. Measurement only creates accountability for the outcomes; the quality of the detailing interaction is what determines whether the activity produces prescribing intent.
Compliance Guardrails: Demand Generation Within the Rules
Prescription demand generation operates within strict regulatory and ethical constraints. Every commercial program must comply with applicable pharmaceutical marketing regulations, and the compliance framework should be built into program design, not added as an afterthought.
On-label promotion only. Every demand generation activity, whether rep-delivered or marketing-supported, must stay within the approved product label. The FDA's Office of Prescription Drug Promotion oversees compliance with these rules. Off-label discussions require a medical affairs pathway, not a commercial pathway, and should never be incorporated into rep detailing programs.
Materials approval processes. All promotional materials used in demand generation programs, including sales aids, patient leaflets, digital content, and speaker presentation decks, must clear the materials approval process before deployment. Rep-generated materials or unofficial adaptations bypass this control and create regulatory exposure.
Interaction logging and transparency. Rep interactions with HCPs must be logged accurately in the CRM, including samples distributed, materials shared, and expenses incurred. In the US, payments and transfers of value to physicians are subject to mandatory disclosure under the CMS Open Payments program, the public database created by the Sunshine Act. Incomplete or inaccurate logging creates compliance risk.
Fair market value for speaker and advisory programs. Speaker programs and advisory boards must compensate HCP participants at fair market value, with rate cards approved by compliance. The PhRMA Code on HCP Interactions sets industry standards for speaker selection, meal limits, and appropriate compensation. Compensation that exceeds fair market value creates anti-kickback exposure regardless of the program's scientific merit.
Building compliance into demand generation program design rather than layering it on afterward keeps the commercial team's programs sustainable, reduces rework, and protects the company's ability to operate in the market long-term. That foundation makes the next step possible: weaving demand generation into the field force's weekly rhythm.
Integrating Demand Generation with the Field Force Operating System
Prescription demand generation doesn't work as a standalone initiative. It works when it's integrated into the field force's weekly operating rhythm: call planning, territory management, CRM hygiene, and performance review.
Reps should enter each call cycle with a demand generation objective for each HCP visit, defined by the HCP's current funnel stage. Call reporting should capture not just that a call happened, but what demand generation activity was executed and what the HCP's response indicated about funnel stage progression.
Field managers should review demand generation metrics in weekly or bi-weekly territory reviews, alongside standard call activity metrics. The questions should be: how many HCPs advanced a funnel stage this cycle? Where are HCPs stalling in the funnel and why? Are script conversion rates tracking at or above benchmark?
When demand generation is built into the operating rhythm this way, it becomes a self-reinforcing system. Reps who see that funnel-stage-appropriate detailing converts HCPs faster become more consistent in their execution. Managers who see territory-level demand generation metrics improving alongside prescription volume understand which rep behaviors drive outcomes.
The field force is the most expensive and most direct demand generation channel available to a pharma commercial organization. Making that channel as productive as possible requires treating demand generation as an operational discipline, measured, managed, and continuously improved, rather than a messaging strategy reviewed once a year at brand planning.
Territories with a structured demand generation system tracking funnel stage advancement per HCP consistently show higher active prescriber growth than territories tracking only call counts and sample distribution, because funnel tracking makes it visible when detailing activity isn't producing prescribing movement and enables earlier intervention.
Patient-directed condition awareness campaigns that encourage patients to seek diagnosis for undertreated conditions generate pull-through demand that complements HCP-facing programs. When patients ask for a specific treatment by name or present with a diagnosed condition, the prescribing conversation starts in a different place than a cold detail.
A demand velocity of 45 to 90 days from first detail to first prescription is a useful planning target for most primary care therapy areas. When velocity extends beyond 120 days, the root cause is often clinical messaging that's too broad rather than a product efficacy problem, and the fix is modular evidence delivery matched to the specific HCP's patient population.
Conclusion
Demand generation is the engine that makes field investment pay off. Sampling without targeting is cost without return. Detailing without funnel-stage awareness is activity without intention. Speaker programs without prescriber pipeline context are brand awareness that doesn't convert to scripts.
The commercial teams that build sustainable prescription volume do so by designing demand generation as a system: a funnel with defined stages, rep-level levers calibrated to each stage, marketing programs that extend field force reach, pull-through mechanics that connect prescribing intent to pharmacy dispensing, and measurement that ties activity to prescription outcomes.
Without this system, sampling and detailing are sunk costs. With it, each field investment compounds over time as HCPs move from awareness to trial to adoption to loyalty, and as loyal prescribers influence their peers to begin the same journey.
Frequently Asked Questions about Prescription Demand Generation
What is prescription demand generation in pharma?
Prescription demand generation is the coordinated set of activities that moves healthcare professionals from awareness of a brand to active, habitual prescribing. It includes field force detailing, sampling programs, speaker events, patient awareness campaigns, and digital content programs. The distinguishing feature of demand generation versus general field activity is that it is funnel-stage-aware: different interventions are applied to doctors at different stages of the adoption process rather than running the same activities for every HCP.
How is demand generation different from traditional HCP detailing?
Traditional detailing treats every doctor call as a delivery of product information. Demand generation treats every call as a deliberate intervention at a specific funnel stage. The difference is in the objective: a detailing call can succeed by delivering a message, while a demand generation call only succeeds if it advances the HCP's prescribing intent. This means demand generation requires pre-call funnel staging, stage-appropriate content selection, and post-call tracking of whether the interaction produced measurable movement.
What's the right script conversion rate benchmark for detailed HCPs?
Conversion rates vary significantly by therapy area, portfolio maturity, and how tightly the target list is defined. For established brands with structured programs and pre-qualified HCP targets, conversion rates meaningfully above 20% are a reasonable goal. Rates persistently below 20% typically indicate a systematic problem in call quality, HCP targeting, or funnel staging rather than a product efficacy issue. Specialty brands with very narrow, pre-qualified HCP lists can achieve higher conversion than broad primary care portfolios.
How do you measure demand generation ROI when prescription data is lagged?
Use leading indicators to track demand generation performance while waiting for prescription data to materialize. The key leading indicators are: funnel advancement rate per cycle (what percentage of HCPs moved at least one stage), sample conversion intent (did the sample placement include a specific patient case discussion), and 48-hour follow-up completion rate for event attendees. These indicators predict the 90-day prescription outcome well enough to allow management intervention before the lagging data confirms the trend.
Should pharmacy stocking happen before or after HCP detailing begins?
Before, or at minimum concurrent with. Creating prescribing intent before nearby pharmacies are stocked produces lost conversions, not delayed ones. Patients who can't fill a prescription at their nearest pharmacy will often accept a pharmacist-suggested substitute, and a substantial portion never switch back to the originally prescribed brand. Field coordination protocols should ensure distribution coverage is secured in a geographic area before the HCP detailing campaign launches in that same area.
What role does digital content play in a demand generation program?
Digital programs (email sequences, webinars, portal-based clinical resources) extend demand generation reach to HCPs who have limited face-to-face access. They work best as a supplement to rep activity, not a replacement: an 8-to-12-week email sequence delivering relevant clinical trial summaries and patient case studies warms HCPs for follow-up rep visits rather than replacing those visits. Digital content that is genuinely educational (not promotional) generates significantly more engagement than brand-forward messaging, particularly in specialty audiences that are skeptical of promotional intent.
Learn More

Senior Implementation Consultant
On this page
- Why Demand Generation Is the Engine of Field Investment Returns
- What Is the Prescription Demand Funnel?
- Demand Generation Levers at the Rep Level
- Marketing-Supported Demand Programs
- Pull-Through Mechanics: Connecting Demand to Dispensing
- Measuring Demand Generation: Connecting Activity to Script Outcomes
- Compliance Guardrails: Demand Generation Within the Rules
- Integrating Demand Generation with the Field Force Operating System
- Conclusion
- Learn More