Service Tier Strategy: Designing Tiered Offerings for Healthcare Practices
Turn this article into takeaways for your work.
Each assistant summarizes the article only for you and suggests best practices for your work.
Healthcare practices often present patients with a binary choice: the covered service or nothing. When insurance pays for a basic exam and the patient needs more comprehensive monitoring, that binary creates a gap. The patient gets less than they need or the practice provides services without compensation.
Service tier strategy addresses that gap. By designing explicit tiers of service at different price and access levels, practices give patients a clearer framework for investing in their own healthcare, create revenue above the insurance baseline, and reduce the awkwardness of explaining upgraded options.
This isn't about upselling patients on unnecessary care. It's about making premium access and more comprehensive services clearly available to patients who want them, with transparent pricing and genuine clinical value at each level.
What Service Tier Strategy Is (and Isn't)
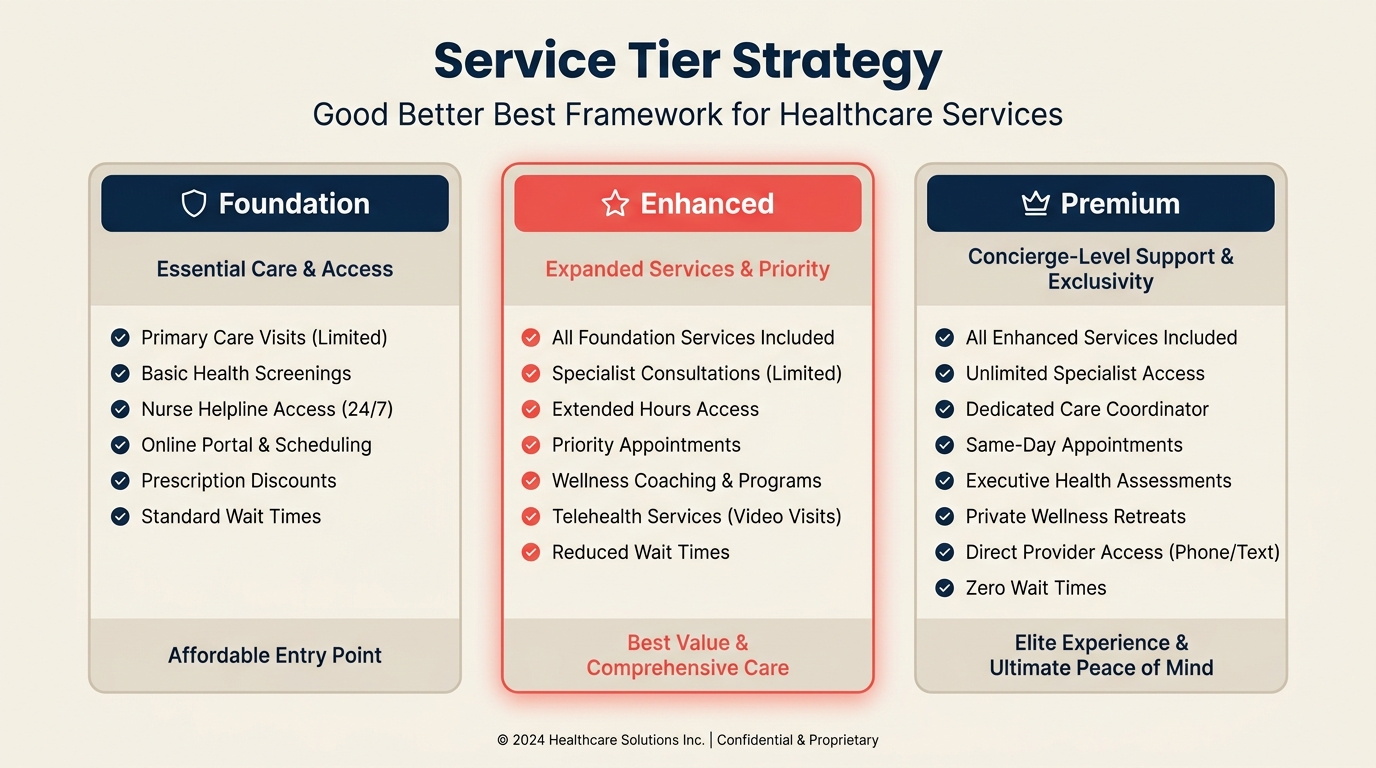
A service tier is a defined package of services, access features, and benefits at a specific price point. Good tier strategies typically have three levels:
- Foundation tier: The baseline service, often insurance-covered or at a lower cash-pay price. Meets core clinical needs.
- Enhanced tier: Added convenience, more comprehensive care, or faster access. A step up from foundation that's available for a modest premium.
- Premium tier: Comprehensive care with the highest access, most proactive monitoring, and the most clinical depth. Positioned for patients who want the best and will pay for it.
The "good/better/best" structure is psychological as much as clinical. When a patient sees three options, they tend to anchor on the middle. Presenting a premium option makes the enhanced tier feel reasonable, not extravagant. That's a well-documented pricing principle across industries, and it works in healthcare too.
What tier strategy is not: medically necessary care should never be withheld because a patient hasn't purchased a higher tier. Tiers are about access, convenience, and comprehensiveness, not gatekeeping required treatment.
Where Tiers Work Best
Service tiers are most effective for:
Preventive and wellness care. Insurance covers a basic annual physical but not comprehensive cardiovascular screening, advanced bloodwork panels, or extended time with a physician for detailed health planning. Patients who want more than the baseline can access it through a premium annual wellness package.
Chronic disease management. A patient with type 2 diabetes might get quarterly visits covered by insurance. An enhanced tier could add monthly check-ins, continuous glucose monitoring support, and direct access to a care coordinator. The foundation tier meets basic coverage requirements; the enhanced tier provides genuinely better care for motivated patients.
Dental and elective services. Dental practices commonly use tiered structures because much care is cash-pay or partially covered. Basic cleaning and exam at one level, comprehensive periodontal care with digital imaging and more frequent visits at another.
Concierge and direct primary care. The concierge medicine model is essentially a full tier structure: membership-based premium access layered above insurance coverage. Even practices that don't want to go full concierge can adopt limited tier elements.
Aesthetic and elective procedures. Practices offering cosmetic or elective services (aesthetics, corrective procedures, weight management programs) naturally suit tier structures because patient investment varies widely and service packages can be meaningfully differentiated.
Designing Your Service Tiers
A well-designed tier structure starts with understanding what patients actually value, not what's cheapest to deliver.
Step 1: List your current services
Document everything your practice offers, both covered and non-covered. Include access features (same-day appointments, direct phone access, portal messaging response time) alongside clinical services.
Step 2: Identify what patients regularly ask for but don't get
Review new patient intake forms, post-visit surveys, and front desk inquiries. What do patients want that you don't currently offer or that isn't standard? Faster scheduling, longer appointment times, results communicated same-day, follow-up calls after procedures, nutritional guidance integrated with medical care?
These requests are your tier design inputs. Patients are telling you what they'd pay for.
Step 3: Define three tiers
Build tiers by grouping services and access features into coherent packages:
Foundation: What your practice delivers to every patient with standard scheduling and standard appointment types.
Enhanced: Foundation plus 2-4 meaningful additions. Might include extended appointment time, guaranteed same-day or next-day scheduling, direct messaging with the care team, and one additional service type not in foundation.
Premium: Enhanced plus the highest-value additions. Might include priority scheduling, unlimited direct access, comprehensive annual wellness assessment, proactive outreach when health markers indicate risk, and a dedicated care coordinator.
The premium tier should feel genuinely different, not just more of the same. Access and responsiveness often matter as much as additional clinical services.
Step 4: Price for value, not cost
Price tiers based on what patients will pay for the value provided, not on your marginal cost to deliver. An enhanced tier that adds genuine convenience and better health outcomes can command a significant premium over foundation even if your direct costs are modest.
For cash-pay tiers, be explicit about what's included. For insurance-integrated tiers, clearly distinguish what insurance covers (foundation) from what the practice charges directly for premium elements.
Treatment Plan Presentation Integration
Service tier strategy and treatment plan presentation are tightly connected.
When presenting a treatment plan, present tier options as part of the conversation. "Your insurance covers the standard protocol. We also offer an enhanced approach that adds X and Y, which many patients in your situation find makes a significant difference. That would be an additional $Z per month." That framing is transparent, non-pressuring, and gives patients a meaningful choice.
The practice needs to be genuinely comfortable with patients choosing foundation. Tier strategy fails if staff treat foundation patients differently or if there's implicit pressure to upgrade. The goal is to make enhanced and premium options clearly available, not to make foundation feel inadequate.
Operational Requirements
Tier strategy only works if the operational infrastructure supports it.
Clear internal definitions. Every staff member should know what each tier includes. Confusion about what's in or out of a tier erodes patient trust quickly.
Documented processes for each tier. Premium patients who expect same-day scheduling need a process that actually delivers that. If operations can't support a tier's promises, don't offer that tier.
Billing clarity. How each tier interacts with insurance billing needs to be spelled out precisely. Financial policy communication to patients about what insurance covers and what comes out of pocket for each tier prevents billing surprises and the patient frustration that follows.
Staff training. Front desk staff need to be comfortable explaining tier options without being salesy. Providers need to be comfortable recommending tiers when clinically appropriate. Scripting helps: "We offer three ways to work with us. Let me walk you through what each includes."
Membership-Based Tiers
A variant on standard service tiers is the membership or subscription model. Patients pay a monthly or annual fee for a tier of care access, regardless of visit frequency.
This works particularly well for:
- Chronic disease management where regular touchpoints add value
- Mental health practices where consistent access matters
- Primary care practices moving toward or experimenting with DPC elements
- Dental practices offering membership plans for uninsured patients
Membership pricing is simpler for patients to understand than visit-based tier pricing. "For $49 a month, you get X, Y, and Z" is easy to evaluate. The practice benefits from predictable revenue and reduced collections complexity.
Dental membership plans are one of the most mature examples of healthcare membership tiers. The model has been refined across thousands of dental practices and offers a useful template for other practice types.
Metrics for Tier Strategy Success
Track the following to assess whether your tier structure is working:
Tier adoption rate: What percentage of patients choose enhanced or premium? A target of 20-30% in enhanced/premium combined is healthy for most practices. Higher means you may be leaving money on the table at foundation. Lower may indicate poor communication or tier design.
Revenue per patient visit: This should increase as tier adoption increases, even holding visit volume constant.
Patient retention by tier: Premium patients typically have higher retention rates. Track whether tier adoption predicts retention.
Case acceptance by tier: When treatment plans are presented with tier options, does overall case acceptance improve? It typically does, because patients feel they have more control over their care investment.
Integrate tier metrics into your regular healthcare practice metrics review.
Common Pitfalls
Too many tiers. Three is the right number for most practices. Four or five creates decision fatigue. Two doesn't create the anchoring effect that makes the middle tier attractive.
Tiers that aren't meaningfully different. If enhanced doesn't feel significantly better than foundation, patients will default to foundation. Each tier upgrade should be worth the premium in ways patients can perceive.
Inconsistent delivery. Premium patients who don't receive what they were promised become the angriest patient complaints you'll face. Under-promise and over-deliver on tier benefits.
Confusion about insurance interaction. Patients need to know exactly what their insurance covers, what the tier membership costs directly, and what they're getting for that cost. Any ambiguity creates billing disputes and distrust.
Applying tiers to everything. Not every service needs tiering. Focus tier development on the services where premium access creates meaningful differentiation and where enough patients are motivated to pay for it.
Key Facts
- The three-tier "good/better/best" structure is psychologically effective: the middle tier gets elevated by the existence of a premium option.
- Service tiers work best for preventive care, chronic disease management, dental, and elective services, where coverage gaps create space for premium value.
- Premium tiers should deliver on access and responsiveness, not just additional clinical services. Faster scheduling and direct access are often what patients value most.
- Membership-based tier structures provide predictable monthly revenue and reduce collections complexity compared to visit-based pricing.
Frequently Asked Questions about Service Tier Strategy
Can service tiers coexist with insurance billing?
Yes. The foundation tier aligns with insurance coverage, and the practice bills insurance normally for those services. Enhanced and premium tiers add services and features not covered by insurance, which patients pay directly. The structure must be clearly disclosed to avoid surprise billing issues.
What if some patients feel pressured to upgrade?
This is a real risk if tier presentation isn't handled carefully. Train staff to present tiers neutrally and affirm that foundation tier meets all clinical requirements. The goal is informed choice, not conversion. Patients who feel pressured don't upgrade; they leave the practice.
How should a practice announce new tiers to existing patients?
Be direct and positive. Explain that you're launching improved care options, describe what each tier includes, and confirm that existing patients' current care isn't changing unless they choose to upgrade. Let patients opt into enhanced tiers rather than auto-enrolling them.
What's the right price differential between tiers?
There's no universal rule, but a 2-3x price ratio between foundation and premium is common in successful tier structures. Foundation to enhanced might be 1.5-2x. The differential should feel proportional to the value difference, not arbitrary.
